This exploratory study provides a comprehensive overview of arrhythmias and structural heart disease in a large cohort of patients with vasculitis. The incidence of ventricular arrhythmias, heart failure with reduced ejection fraction, acute myocardial infarction, and cardiomyopathy was low with less than seven percent in the overall population experiencing these potentially life-threatening events after vasculitis diagnosis. Yet, our analysis also demonstrates that cardiovascular risk factors, cardiac symptoms, and less severe structural abnormalities affect a substantial proportion of patients with vasculitis, highlighting the potential to reduce cardiac morbidity through systematic screening and multidisciplinary management.
The differences between the five main subgroups at baseline, i.e., at the time of vasculitis diagnosis, pose a challenge for the interpretation of this study. Some of these differences are directly related to the diagnostic criteria for specific disease subtypes. For example, age below 60 years is considered an absolute requirement for the diagnosis of TAK, while age of ≥ 50 years is a prerequisite of GCA, according to the 2022 American College of Rheumatology (ACR)/EULAR classification criteria [20, 21]. Further, asthma is a typical early clinical feature of EGPA and an important diagnostic criterion, and in accordance with the high rate of chronic pulmonary disease observed at EGPA diagnosis in our study [15, 24]. The high prevalence of arterial hypertension at baseline among patients with GCA may in part be age-related, but may also be an early manifestation of increased arterial wall stiffness due to aortic involvement [25]. Imbalances of non-modifiable and modifiable cardiovascular risk factors at the time of vasculitis diagnosis, knowledge gaps regarding the specific pathomechanisms of cardiac involvement, and the complex interplay between immunomodulatory medications and cardiovascular risk complicate comparisons between these heterogeneous patient subgroups.
A salient finding of the present study was the relatively high rate of LV systolic dysfunction and myocardial fibrosis after EGPA diagnosis compared to other vasculitis subtypes. The risk of cardiac involvement is known to be more pronounced in ANCA-negative EGPA patients [26,27,28,29,30]. In a French multicenter analysis of 383 EGPA patients, 16.4% had cardiomyopathy at the time of diagnosis [26]. In another prospective study involving 50 EGPA patients, comprehensive cardiologic screening using clinical assessment, laboratory analysis, electrocardiogram, echocardiography, and CMR revealed cardiac involvement in 66% of patients [7]. Importantly, EGPA patients with cardiac involvement had a higher risk of death during the mean follow-up period of 53 months [7]. Other analyses have demonstrated that cardiac involvement commonly affects asymptomatic patients [29]. The observational design of our study did not allow for the detection of subclinical cardiac disease but aligns with previous findings highlighting the high prevalence of cardiac morbidity in EGPA patients [7, 26,27,28,29,30,31,32,33]. Thus, our data also supports the call for incorporating cardiologic screening tests including imaging into the routine diagnostic workup at EGPA diagnosis [15]. Whether or not CMR should be part of a standard screening algorithm remains a matter of debate. In a recent study focusing on CMR findings, the sensitivity of elevated N-terminal pro-B-type natriuretic peptide (NT-proBNP) and Troponin T for cardiac involvement, i.e., focal or multifocal subendocardial LGE, was 38% and 56%, respectively [32]. Evidence regarding the value of repeated imaging and EMB is also scarce. Additional information from longitudinal studies including a detailed analysis of inflammatory disease markers at the time of overt and subclinical cardiac involvement is needed to better understand the pathophysiology and chronicity of structural changes, and to guide clinical management.
Stenotic coronary artery disease was excluded in all seven EGPA patients enrolled in this study who underwent coronary angiography. By contrast, acute myocardial infarction requiring PCI was documented in four GCA patients corresponding to a prevalence of 3.7% over a median follow-up period of 36 months. Although GCA patients appeared to have an increased risk of major adverse cardiovascular events due to the presence of baseline risk factors in our cohort, systemic inflammation, coronary vasculitis, and side effects of immunomodulatory medications may have contributed to myocardial ischemia, as well. Two independent healthcare database analyses conducted in Canada and the UK found a significantly higher incidence rate of myocardial infarction and stroke among GCA patients compared to non-GCA controls after matching for age and sex [9, 34]. In a study by Greigert et al., the incidence of myocardial infarction in a cohort of 251 biopsy-proven GCA patients was 5.2% [35]. Of the 13 total events, the authors classified six cases of myocardial infarction as GCA-related, defined by their occurrence within three months before or after a GCA flare [35]. Interestingly, patients who experienced GCA-unrelated myocardial infarction more often had extensive coronary artery disease and type I myocardial infarction, and tended to have received antiplatelet therapy more frequently prior to the event [35]. In the present cohort, coronary lesions other than atherosclerotic were detected in two patients with GCA and GPA, respectively. Few case reports have described coronary arteritis as a rare complication of GCA, whereas it is more frequently observed in TAK, with coronary involvement reported in up to 53% of cases [10, 36,37,38,39,40,41]. In GPA, coronary artery aneurysm and dissection have been described in rare cases [42,43,44]. These observations underscore the complexity of coronary artery involvement in vasculitis and the challenge of reliably estimating the risk of major adverse events in clinical practice. In fact, the 2022 EULAR recommendations for cardiovascular risk management in rheumatic diseases acknowledge, that disease-specific factors may impair the accuracy of traditional risk prediction tools [18]. However, due to the lack of validated alternative models, these established tools remain recommended for vasculitis patients, except in ANCA-associated vasculitis, where the European Vasculitis Society (EUVAS) model should be considered [18].
Inflammatory disease activity has been demonstrated to correlate with cardiovascular risk in ANCA-associated vasculitis [45, 46]. In GCA and TAK, the use of adjunctive immunosuppressive/immunomodulatory medication has been shown to be associated with a reduced rate of cardiovascular events, including stroke and myocardial infarction [47, 48]. Apart from the GCA subgroup, almost all study participants received disease-modifying anti-rheumatic drugs over the disease course. This finding reflects general efforts to implement corticosteroid-sparing agents for vasculitis management but may also be influenced by the recruitment of patients for clinical trials at our university-affiliated tertiary center. Since laboratory markers were not collected in this study, adjudicating major cardiovascular events based on disease activity was not feasible. Thus, we can only speculate that individualized medication management could have contributed to the overall low event rate and attenuated the risks associated with long-term corticosteroid use. A notable result from our analysis of cardiovascular medications was the high proportion of GCA and TAK patients receiving or having previously received platelet inhibitors after a vasculitis diagnosis, possibly because their use for primary prevention in large vessel vasculitis was recommended until 2020 [13, 18, 49]. Besides, patients with LV systolic dysfunction should ideally be treated with a combination of four heart failure medications, if tolerated [23]. However, not all patients with reduced LV ejection fraction had been prescribed an aldosterone antagonist or an angiotensin receptor-neprilysin inhibitor. These findings highlight the importance of multidisciplinary management in preventing overtreatment and optimizing long-term medication plans.
Owing to the variety of initial symptoms and organ manifestations, vasculitis was often diagnosed months -or even years- after symptom onset in the present cohort. In a previous survey of 456 vasculitis patients, 73% were initially misdiagnosed, with a median time of seven months between the onset of symptoms and diagnosis [50]. The range of clinical specialists involved in the diagnosis reflects these challenges and underscores the importance of cardiologists considering these rare diseases, particularly in younger patients with atypical cardiac conditions and suggestive inflammatory comorbidities [51].
Limitations
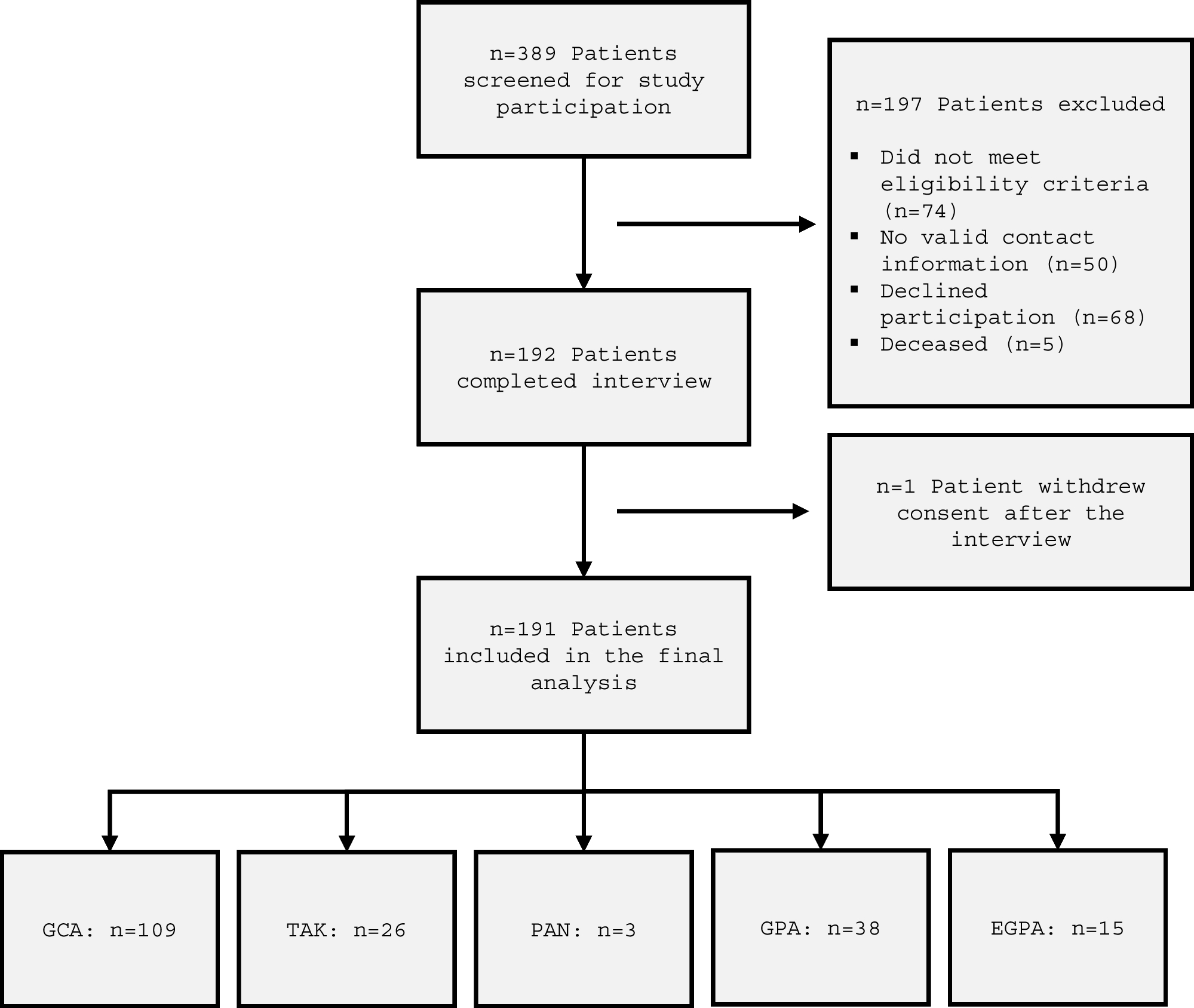
Main limitations of the present analysis are related to the retrospective study design and the potential biases associated with interview-based data acquisition. Self-reported data may be subject to recency and recall bias, potentially affecting the accuracy of symptom onset, the time of diagnosis, medication history et cetera. However, this information was double-checked on the basis of clinical records. Since deceased patients were excluded by study design, those with severe cardiac manifestations or comorbidities may have been underrepresented. Given the very small number of patients with PAN, the estimated incidence of cardiac conditions may be unreliable and regression analyses were not feasible due to marked group size imbalances. The timing of cardiovascular events in relation to vasculitis diagnosis was not analyzed, which may have introduced additional bias due to variability in follow-up durations. Lastly, as patients were recruited from a major university hospital with specialized rheumatology and angiology departments, the findings may not be generalizable to other settings.



Comments (0)