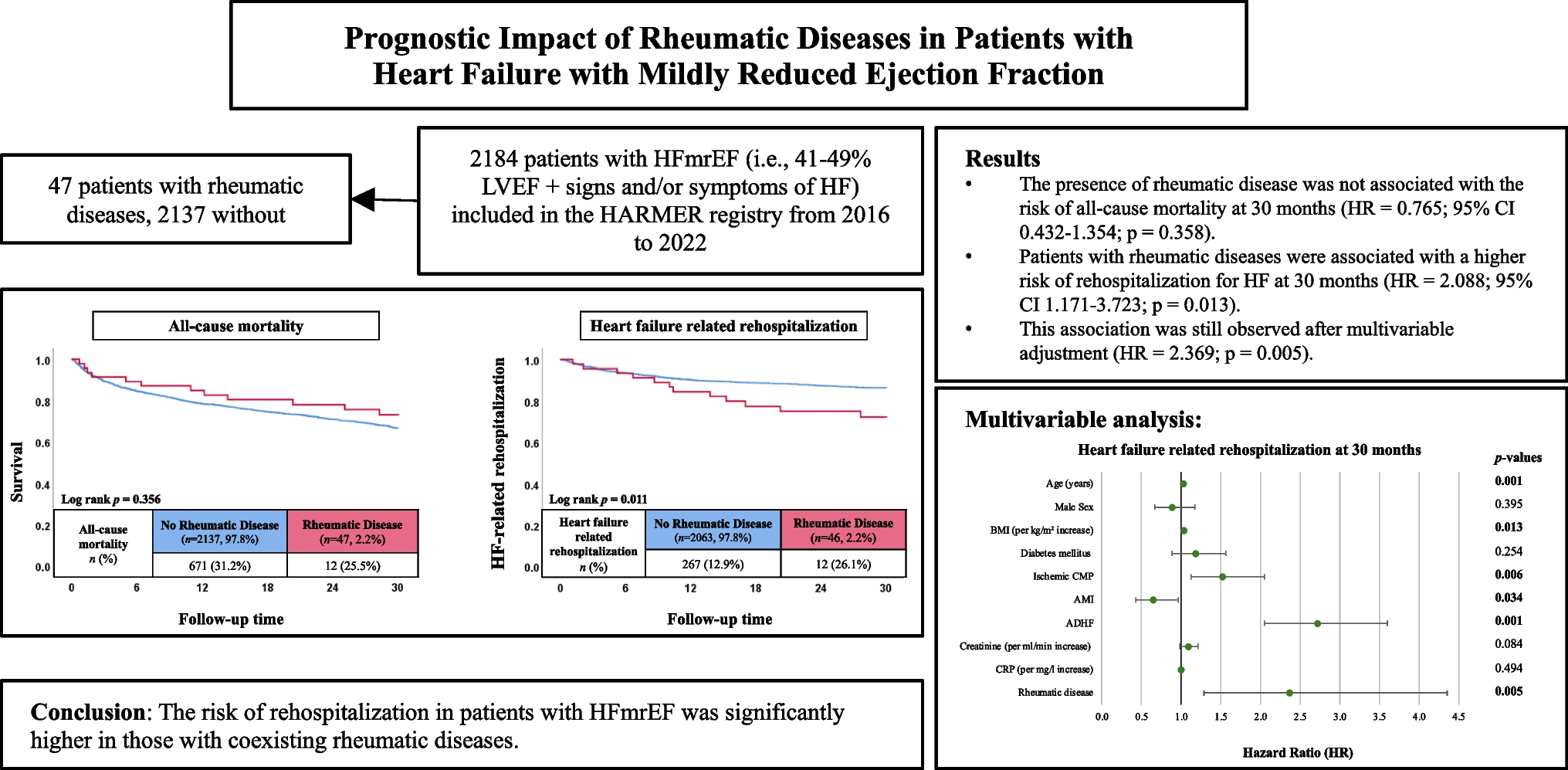
This study aimed to examine whether concomitant rheumatic diseases impact long-term prognosis of patients with HFmrEF. The findings suggest that patients with HFmrEF and coexisting rheumatic diseases experience higher rates of HF-related rehospitalization compared to those without rheumatic comorbidities. Multivariable analysis confirmed that the presence of rheumatic disease is an independent predictor of rehospitalization in patients with HFmrEF. In contrast, no significant difference in all-cause mortality was observed over a 30-month follow-up period between patients with and without rheumatic diseases. The proportion of patients with rheumatic disease in this cohort (2.2%) is consistent with its estimated prevalence in the general population [9], supporting the representativeness of the sample.
Numerous large-scale studies have consistently demonstrated an association between rheumatic diseases and increased mortality. For instance, a retrospective observational cohort study conducted in the United Kingdom, encompassing over 2.3 million individuals, found that patients with RA exhibited significantly higher risk of all-cause mortality, along with elevated rates of both fatal and non-fatal vascular events, when compared to the general population [11]. Furthermore, a comprehensive meta-analysis of 24 cohort studies reported that individuals with RA face a 50% higher risk of cardiovascular disease-related mortality relative to those without RA. These findings underscore the substantial cardiovascular burden associated with chronic inflammatory rheumatic conditions [10].
Despite this well-established association between rheumatic diseases and elevated cardiovascular and all-cause mortality, the present study did not find a significant difference in mortality during the follow-up period of 30 months between HFmrEF patients with and without rheumatic diseases. This discrepancy may be attributable to the relatively small number of patients with rheumatic diseases in our cohort, as well as the heterogeneity of conditions within this group. However, patients with rheumatic diseases had a significantly higher risk of HF-related rehospitalization, even after multivariable adjustment.
In line, a retrospective analysis using the U.S. Nationwide Readmissions Database (NRD), which included all patients hospitalized for HF, demonstrated that individuals with a concurrent diagnosis of rheumatoid arthritis (RA) had a higher likelihood of being readmitted within 90 days of their initial hospitalization [13]. Similarly, another study found increased rehospitalization rates in patients with AMI who also had systemic lupus erythematosus (SLE), compared to those without SLE [14]. These findings reinforce the notion that rheumatic diseases may contribute to a more complicated clinical course in patients with cardiovascular conditions.
Various studies have established, that several inflammatory biomarkers – such as IL-6, TNF-α and CRP – play a key role in the prediction of cardiovascular events and are associated with increased mortality in patients with cardiovascular diseases [15,16,17,18]. Notably, these same biomarkers are critically involved in the pathophysiology of rheumatic diseases, including RA [8, 19, 20]. This overlap may help explain the increased clinical burden observed in patients with both conditions.
Another observation that could be drawn from our results is the differential pattern of risk predictors identified in the multivariable analysis. Among patients with rheumatic disease, ADHF emerged as the sole independent predictor of both mortality and rehospitalization. Whereas traditional cardiovascular risk factors such as age, BMI, diabetes, and renal function were not significantly associated with either outcome. In contrast, in patients without rheumatic comorbidities, a broader range of variables were significantly linked to adverse outcomes. This discrepancy may reflect the overriding influence of systemic inflammation and immune dysregulation in patients with rheumatic disease or could be attributed to low case numbers in the rheumatic disease group.
It is important to acknowledge that the majority of patients with rheumatic diseases are typically treated with specific pharmacological therapies that may influence outcomes in the presence of concomitant HF. In our cohort, nearly half of the patients within the rheumatic disease subgroup (n = 20; 42.6%) were receiving glucocorticoids, which have been associated with an increased risk of HF and other adverse cardiovascular events in previous studies [5]. Additionally, 9 patients (19.1%) were prescribed conventional synthetic disease-modifying antirheumatic drugs (csDMARDs), a medication class that has generally demonstrated a neutral or even protective cardiovascular profile. Notably, methotrexate as one of the most commonly used csDMARDs has been linked to improved cardiovascular outcomes in several previous studies [21]. Given the increased risk of HF-related rehospitalization in HFmrEF patients with rheumatic diseases, the prognostic impact of disease-modifying antirheumatic drugs on recurrent HF patients warrants further investigation, specifically in patients with recurrent decompensated HF.
In addition to our findings concerning major endpoints, two notable secondary observations emerged from the present analysis. First, patients in the rheumatic group revealed a significantly lower heart rate with a median of 72 bpm compared to those without such conditions (80 bpm). This finding is consistent with research indicating reduced heart rate variability in individuals with chronic inflammatory diseases. According to several studies, subclinical inflammation increases sympathetic activity and reduces parasympathetic (vagal) tone at the same time [22, 23]. These negative effects on the autonomic nervous system function are knowingly connected to worse outcomes, such as higher mortality in patients with progressive HF [22]. This finding may contribute to explaining the increased rates of rehospitalization observed in patients with rheumatic diseases. Their diminished capacity to adequately respond to physiological challenges – particularly those requiring sufficient heart rate variability and intact autonomic nervous system function – may predispose them to more rapid cardiovascular decompensation.
Second, patients in the rheumatic disease group were more frequently prescribed loop diuretics upon initial hospital admission. This prescribing pattern corresponds with a slightly higher prevalence of chronic kidney disease (CKD) noticed in the same group. This observation may be attributed to shared underlying inflammatory mechanisms, as both rheumatic diseases and CKD are driven, at least in part, by chronic systemic inflammation [24, 25]. Such overlapping pathophysiological pathways likely contribute to the frequent co-occurrence of these conditions in clinical practice. These findings suggest a greater burden of comorbidity in patients with rheumatic disease, which may partly explain their increased rates of rehospitalization.
Regardless of the underlying causes driving higher rehospitalization rates among patients with both rheumatic diseases and HFmrEF, the increased frequency of hospital admissions in this population represents a substantial burden on our healthcare system. HF is among the leading causes of hospitalization in Germany, accounting for a significant proportion of inpatient admissions each year. Notably, more than two-thirds of the total healthcare costs related to HF are incurred through inpatient care alone [26]. Frequent hospitalizations also negatively impact patients themselves, as each readmission increases the risk of nosocomial infections and physical deconditioning and with that all-cause and cardiovascular mortality [27]. To mitigate these challenges for both patients and the healthcare system, further research is needed to better understand the interplay between HFmrEF and comorbidities, particularly rheumatic diseases.
Finally, further robust research such as observational prospective studies should continue to explore the similarities and differences in the phenotypes of patients with HF across different LVEF thresholds. Such groundwork is essential to more precisely identify the unique characteristics of patients with HFmrEF, which could ultimately enable more tailored diagnosis strategies and therapeutic approaches.
Study limitations
The retrospective and single-centre study design need to be considered as main limitations. Diagnostic thresholds and definitions of rheumatic diseases could not be standardized and unknown confounders may have influenced the results. The number of patients with rheumatic diseases was low. Due to the small sample size, all rheumatic conditions were analyzed as a single group and no further risk stratification was performed stratified by different rheumatic diseases. Given the heterogeneity in pathophysiology and organ involvement among rheumatic diseases, it remains unclear whether they exert uniform effects in patients with HFmrEF. Since measurements on longitudinal left ventricular function was performed in minor part of the study cohort, those measurements were beyond the scope of the present study. The study cohort included patients with HFmrEF only, the prognostic impact of rheumatic diseases in patients with HFpEF and HFrEF was beyond the scope of the study.



Comments (0)