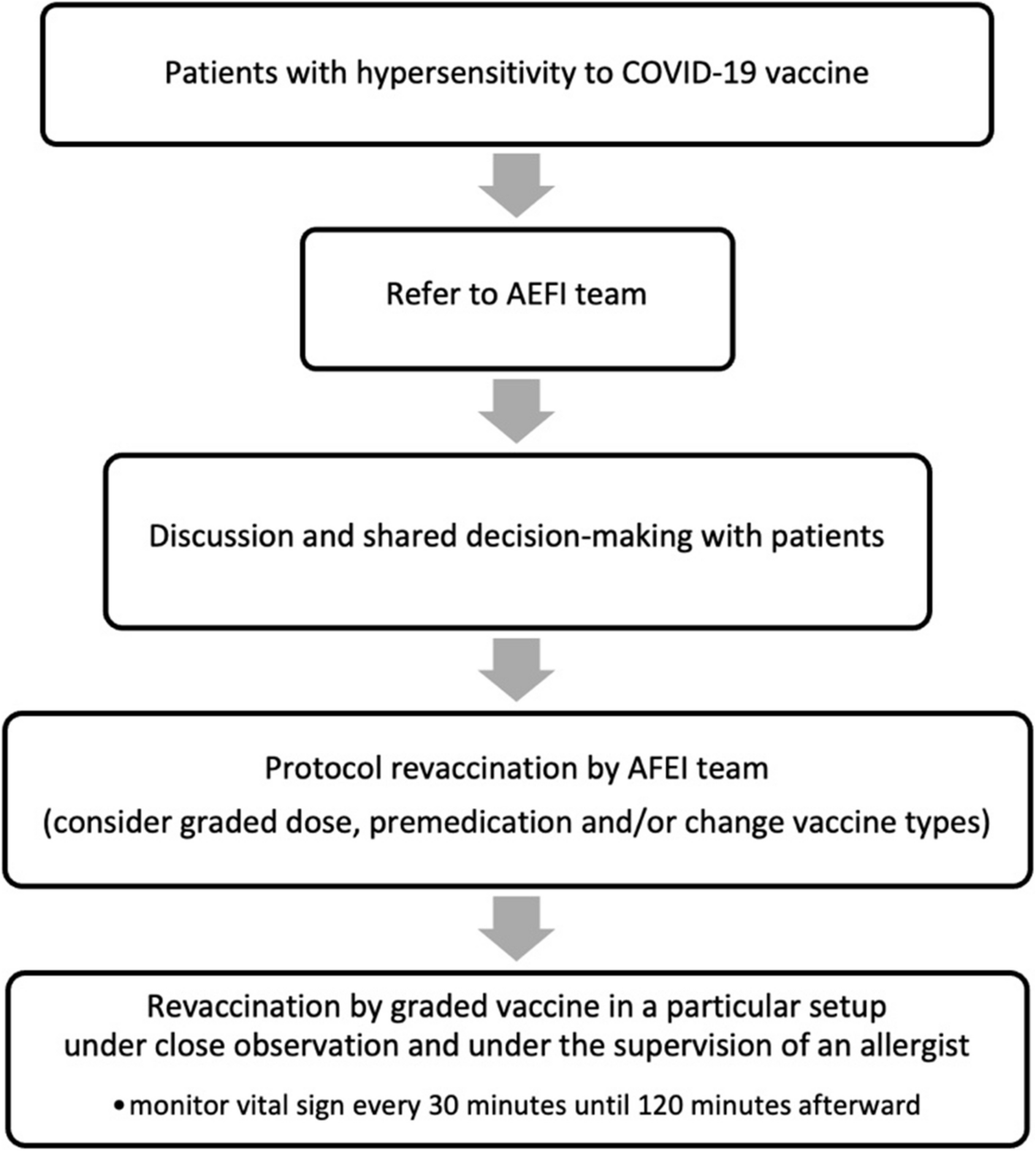
The development of COVID-19 vaccines has been a critical milestone in the ongoing effort to combat the SARS-CoV-2 pandemic. However, vaccine hesitancy has been a major concern among both healthcare providers and the general public since the inception of the COVID-19 vaccination campaign. To effectively manage this issue, Songklanakarind hospital has established an AEFI team with the primary objective of evaluating patients who have experienced Adverse Events Following Immunization in response to COVID-19 vaccines.
In our cohort, 225 subjects were assessed because they had HSR to COVID-19 vaccine, 175 of whom already had revaccination. We aimed to investigate the occurrence of HSR to the COVID-19 vaccine, focusing specifically on allergic reactions and revaccination outcomes. A total of 1,386 patients were referred to this center, and 16% were found to have allergic reactions. According to a study in Turkey, CoronaVac vaccination resulted in mild allergic reactions, such as skin rashes (2.3%) and urticaria (0.8%) [3]. On the other hand, in the US, the reported incidence of mild allergic reactions for Pfizer and Moderna was 1.9% and 2.2%, respectively [5]. Our study found that anaphylaxis occurred at a rate of 0.5%. In the US, severe allergic reactions were reported at rates of 0.00047% and 0.00025% administered for Pfizer and Moderna, respectively. In another US study, allergic reaction or anaphylaxis was reported in 0.3% of participants after partial vaccination and 0.2% of participants after full vaccination [17]. Our study is criticized for not including all vaccine recipients in its survey since it only looked at the group that had received counseling when symptoms appeared. Interestingly, the study focused mostly on allergic reactions, notably urticaria, a common and apparent symptom. As a result, it appears that more allergic reactions were reported in this study than in the previous study. The study's limitations must be taken into consideration when evaluating its results.
In this study, most patients who had HSR are female. Similar to previous studies [13,14,15,16] have reported a higher frequency of AEFI among women. In addition, a study conducted by Rajneesh K. Joshi et al. [17] revealed that female was a significant independent risk factor for systemic AEFI reported after COVID-19 vaccination, with an adjusted RR of 2.24 (95%CI: 1.22–4.09) [18]. Recent systematic review and meta-analysis showed 87.8% of women had immediate allergic reactions to their first vaccination [19]. Additionally, a study by Chiang et al. demonstrated a disproportionate rate of female referrals for suspected COVID-19 vaccine allergies, further supporting the higher incidence of AEFI in females. [20]
The study was conducted between April 2020 and August 2022, during the initial phase of the study, the most used vaccine was the inactivated vaccine, which resulted in a higher incidence of hypersensitivity reactions compared to other vaccines that were introduced later.
The World Allergy Organization (WAO) recommends that individuals who experience a systemic allergic reaction to a vaccine should not receive a second dose of that vaccine, nor a vaccine with similar excipients [21]. Nonetheless, there have been several reports of successful revaccination with the same platform after experiencing an immediate hypersensitivity reaction to the first dose [7, 22,23,24,25,26,27,28]. It is important to note that the decision regarding revaccination may vary depending on a number of factors, including the specific vaccines that are available and the protocols for vaccination in a particular country or region. In the case of Thailand, for example, the protocols for revaccination may vary depending on the severity of the reaction and the availability of alternative vaccines. According to the vaccine available, individuals who experience an allergic reaction to a COVID-19 vaccine may be able to receive a second dose of the same vaccine, with close monitoring for any adverse reactions. However, individuals who experience a more severe allergic reaction may be advised to receive an alternative vaccine, if available, or to defer revaccination until more information is available.
There are varying recommendations from international organizations regarding the use of premedication with antihistamines in individuals with prior vaccine-related allergic reactions. The World Allergy Organization (WAO) cautions that antihistamines may mask early cutaneous signs of anaphylaxis, potentially delaying recognition and appropriate treatment [21]. Similarly, the American Academy of Allergy, Asthma & Immunology (AAAAI) notes this concern but allows that second-generation antihistamines such as cetirizine or fexofenadine may be considered in patients with a history of mild symptoms like isolated urticaria or pruritus [1]. In contrast, the British Society for Allergy & Clinical Immunology (BSACI) and the Korean Academy of Asthma, Allergy and Clinical Immunology (KAAACI) suggest that premedication may reduce symptom severity and improve patient confidence during revaccination [23, 24, 28, 29]. In our setting, premedication with antihistamines—alone or in combination with anti-leukotrienes—was used in 63.4% of patients. This institutional practice was guided by clinical experience and the intention to reduce mild hypersensitivity symptoms, particularly in those with previous urticaria or non-severe cutaneous reactions. While we acknowledge that premedication is not universally endorsed and may not prevent anaphylaxis, our protocol emphasized patient selection, risk stratification, and close post-vaccination monitoring to mitigate potential masking effects.
The outcome of revaccination in our study, all patients can receive revaccination, 10.9% had a mild adverse reaction. Same as in a systematic review and meta-analysis, 232 developed mild symptoms (13.65%), and, conversely, 1360 tolerated the dose (99.84%), Most can tolerate well, with only a small proportion experiencing mild adverse reactions [19]. We compare the characteristics of patients who experienced adverse reactions following revaccination with those who did not exhibit any adverse reactions. Between group comparison indicated a significant association among patients with post vaccination adverse effects, in particular when revaccinated with inactivated vaccines, in the presence of a history of any allergic diseases and especially in regard to allergic rhinitis, versus any other specific allergic disease examined. These findings suggest that individuals with a history of allergic disease, particularly allergic rhinitis, should be closely monitored during revaccination with inactivated vaccines to prevent adverse reactions. Further research is needed to elucidate the underlying mechanisms responsible for the increased risk of adverse reactions in this population.
This study has some limitations, including the observational retrospective design and the single-center analysis, further, the number of patients with HSR was relatively small. Also, due to restrictions on the provision of vaccinations at the time of our study, we were unable to perform SPT or IDT to investigation. Moreover, we grouped urticaria and angioedema together due to their clinical overlap and frequent co-occurrence. However, this approach has limitations as they are distinct manifestations. Another limitation is our reliance on patient-reported histories or medical records to identify allergic diseases, including drug allergies. This may not accurately reflect true allergy status, as many individuals with drug allergies may be misdiagnosed. Previous studies, such as Kan et al., have highlighted that a significant proportion of drug allergy labels, particularly in the context of COVID-19 vaccines, are incorrect and could be addressed through allergy evaluation and delabelling services [29]. This underlines the need for objective diagnostic testing to confirm allergic conditions in future research. Finally, further studies are needed to explore the potential benefits and drawbacks of premedication with antihistamines in patients with a history of potential allergic reactions to any COVID-19 vaccination platforms, as well as to investigate the underlying factors contributing to the elevated risk of adverse reactions in this population.



Comments (0)