
Remember me


The study was conducted at health centers in Konso Zone, South Ethiopia, which is about 595 km south-west of Addis Ababa. The zone comprises four woredas with 43 kebeles, of which 41 are rural kebeles. The total population of the zone is 318,819; of these, 153,903 are men and 164,916 are women [25]. The zone consists of 13 health centers and two primary hospitals that provide primary health services to the community. Geographically, it is located at 5o 12′ − 5o 40′ N latitude and 37o 01′ − 37o 43′ E longitude. The area’s elevation ranges from 501 to 2000 m above sea level, with a total land area of 2,016.24 km2 [26].
Study design and periodA case control study design was conducted from April to July 2024 in health centers in Konso Zone, South Ethiopia.
Source of populationFebrile individuals visited the outpatient department (OPD) at health centers during the data collection period.
Study participants Case groupAll untreated malaria patients who were confirmed as positive for P. falciparum during the data collection period.
Control groupFebrile individuals visited the OPD in the health centers who were confirmed as negative for malaria infection during the data collection period.
Eligibility criteria Inclusion criteria for case groupAll untreated malaria patients positive for P. falciparum and willing to participate in the study were included.
Inclusion criteria for the control groupSubjects who were febrile and negative for malaria and have not received any treatment yet.
Exclusion criteria for case and control groupsParticipants with preexisting cases of diabetes mellitus, hypertension, kidney disease, liver disease, heart disease, and cancer were excluded. Alcohol, smoking, and an individual’s use of medication were also excluded from the study.
Determination of sample sizeThe estimated percentages for the exposed group were 16.2%, based on a systematic review and meta-analysis study conducted in Ethiopia in 2021 [27], and 50% was taken into account for the control group. We determined the study’s sample size using a 95% confidence interval (CI), a 5% margin of error, a 2 design effect, and an 80% power of test. The sample size selection for cases and controls was a 1:1 ratio. The sample size is calculated using the case-control formula, and n = 54 for each group. Thus, the total sample size is 108.
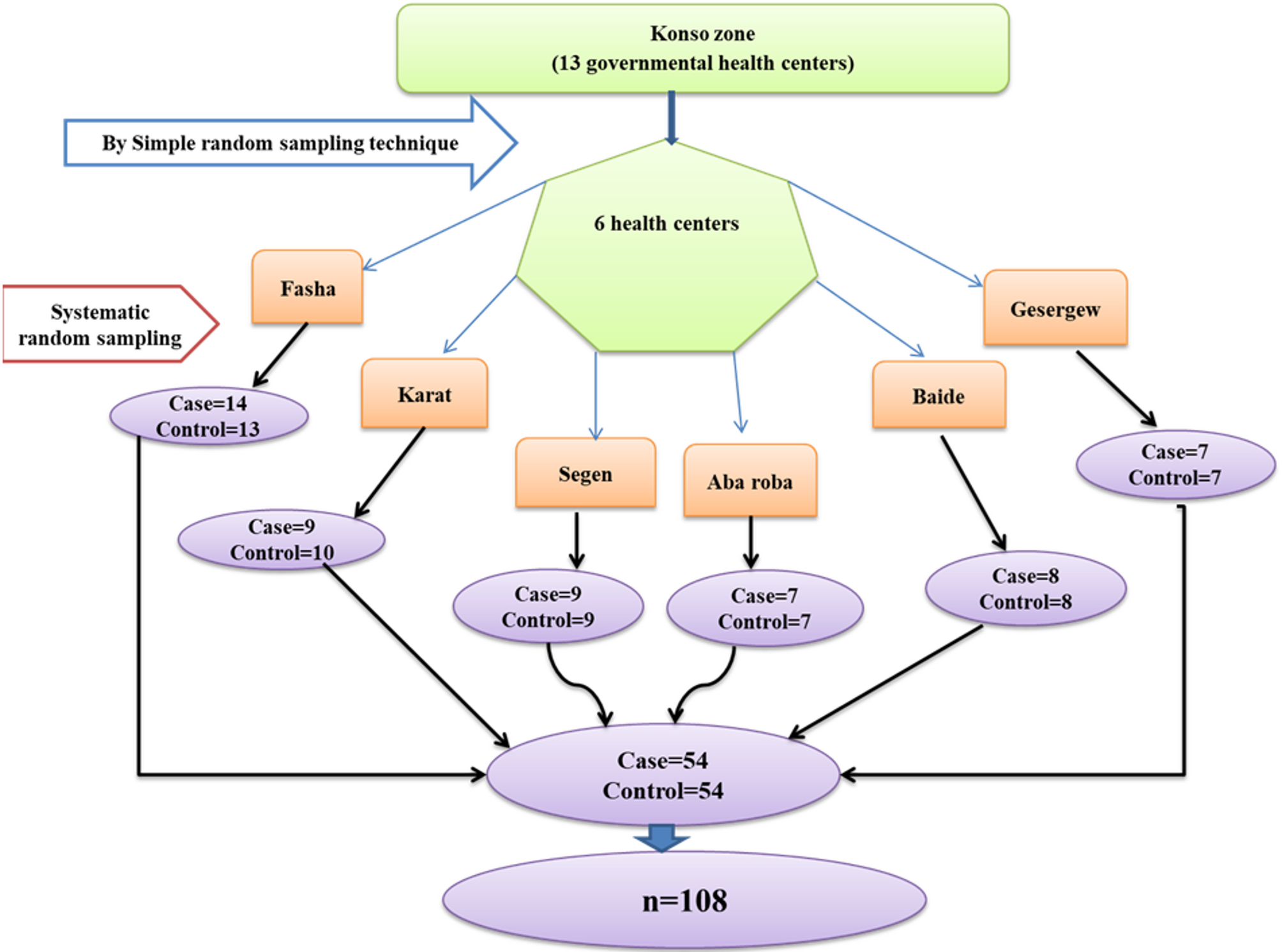
Sampling techniqueA multistage sampling technique was used in this study. First, 6 health centers were randomly selected from a total of 13 health centers in the Konso zone by a simple random sampling technique. Then, the sample size of each group was proportionally allocated to the selected health centers based on the size of the total number of study participants in each health center (Fig. 1). Subjects who had malaria in the case were selected as the case group. Non-malaria and volunteer subjects were taken as a control group. A systematic sampling technique was used to select participants in each health center.
Fig. 1
Schematic representation of sampling techniques to select study participants in health centers, Konso Zone, South Ethiopia
Study variables Dependent variablesCreatinine, urea, Na+ and K+.
Independent variablesSocio-demographic characteristics such as age, sex, marital status, educational status, residence, occupation, body mass index (BMI) and blood pressure.
Data collection materialsStructured interview questionnaires, a blood pressure apparatus (sphygmomanometer), a stethoscope, measuring tape, weighing and height measuring scales, a finger prick, a microscope, a Nanc or Eppendorf tube, and a 5 cm³ syringe were used for data collection.
Data collection and measurement proceduresTo choose the eligible participants for the study, the following steps were taken: The purpose of the study was explained in an initial meeting with the directors of the health centers in the Konso zone. The researcher provided half-day training to each data collector prior to the actual start of data collection. The purpose of the study was explained to study participants, and both verbal and written consent was sought. Information confidentiality was guaranteed during the whole study process. Each participant had a 5 ml venous blood sample drawn for a kidney function examination and serum electrolyte evaluation, and data were gathered via a questionnaire.
Standard operating proceduresQuestionnaireA standardized questionnaire was created before the trial began specifically to collect sociodemographic information and measure the participants’ blood pressure, height, and weight. A standard questionnaire was used to collect all pertinent personal data, with non-malaria and consenting volunteers serving as the control group and malaria-susceptible individuals proven to have P. falciparum infections as a case.
BMI and blood pressure measurementThe weight of the participants was measured in kilograms (kg) with light clothes and without wearing shoes, and their height was measured in meters (m) using a height board without shoes in an upright position. Then, BMI was calculated by dividing weight in kg by height squared in m2; BMI = weight (kg)/height2 (m2). The study participants were considered underweight when their BMI is < 18.5 kg/m2, normal when their BMI is 18.5–24.9 kg/m2, overweight when their BMI is 25–29.9 kg/m2, and obese when their BMI is ≥ 30 kg/m2 [28].
After participants have rested for at least thirty minutes, for those who take hot beverages such as coffee, their blood pressure was monitored using an automated digital blood pressure measuring instrument (sphygmomanometer) in the middle of their left arm in accordance with WHO recommendations. Each participant had three blood pressure readings obtained; the true value was determined by taking the average [29]. The mean blood pressure ≤ 89/59 mmHg was defined as low/hypotension, 90/60–139/89 mmHg was defined as normal, and ≥ 140/90 mmHg was defined as high/hypertension by systolic/diastolic, respectively.
Blood sample collection and processingCapillary blood samples were aseptically obtained by fingerprick in order to form a thin blood film that could be used to identify and detect Plasmodium species using pre-labeled microscope slides. After staining the prepared blood films for ten minutes with a 10% Giemsa solution, they were left to air dry at room temperature. A high magnification power objective (100X) of the microscope was used to observe the blood film after the stained slides had air-dried.
About 5 ml of blood was drawn from the antecubital vein using a 5 cm3 syringe by a laboratory technologist from both untreated malaria patients and non-malaria controls. The blood from each participant was collected in a serum separator tube. Then, after 30 min, blood samples were centrifuged at 4000 revolutions per minute for five minutes, and serum samples were harvested into Eppendorf tubes. Following serum separation, it was stored in a deep freezer until the analysis was done.
Sample processing and test principlesDetermination of serum creatinineThis procedure is based upon a modification of the original picrate reaction (Jaffe) [30]. Creatinine was analyzed using the Jourilabs kinetic method performed with a semi-automated chemistry analyzer DR-7000D (Dirui Industrial Co., Ltd., Changchun, Jilin 130103, and P.R. China).
Determination of serum UreaUrea was analyzed based on the Jourilabs enzymatic method by a semi-automated chemistry analyzer DR-7000D (Dirui Industrial Co., Ltd., Changchun, Jilin 130103, and P.R. China) [31].
Determination of serum electrolytes (Na+ and K+)Serum Na+ and K+ levels were estimated with the Cobas 6000 (Roche Diagnostics International Ltd., CH-6343 Rotkreuz, Switzerland). Photometric and ion-selective electrolyte results are combined to optimize the Cobas 6000 analyzer series for workloads. The ion-selective electrolyte system is used in the quantitation of electrolytes (Na+ and K+) [32].
Data quality managementData collectors were trained professionals to ensure consistency and reduce intra- and inter-observer variations. Close supervision was provided by the researcher throughout the data collection. The collected data was checked for completeness, accuracy, and consistency. All laboratory machines were checked for their proper function before analyzing samples.
Data entry and analysisData collected were coded, entered into a computer, cleaned, and managed by SPSS version 27 for analysis. The data was summarized using the descriptive statistics with a standard deviation (SD). Categorical variables were presented in frequency and percentage, while continuous variables were presented as mean ± SD. The data output was interpreted using tables. The odds ratio was measured with 95% CIs to quantify the strength of association between the case group and the control group. Variation analysis between the case group and control group was conducted using one-way ANOVA. The difference in the mean among groups was analyzed by an independent sample T-test. The correlation between the variables was displayed using the Spearman’s rho correlation coefficient. Statistical significance was decided when P < 0.05.
Operational definitions Untreated malaria patientsAn individual infected with the malaria parasite does not receive any form of medical intervention or treatment to combat the infection.
AKIAn abrupt decrease in kidney function, manifested by an increase in serum creatinine and urea and in the dysregulation of extracellular volume [33].
Hypercreatinaemia: The serum creatinine level greater than the reference value (reference value: 0.7–1.3 mg/dL for males and 0.6–1.1 mg/dl for females).
Hyperuraemia: The serum urea level greater than reference value (reference value: 18–45 mg/dL).
Hyponatraemia: Decreasing of Na+ level (reference value: 136–145 mmol/L) [34].
Hypokalaemia: Decreasing of K+ level (reference value: 3.5–5 mmol/L) [34].
Comments (0)