
Remember me




We performed RCT pilot study (clinicaltrials.gov: NCT02976558, first registration 29.11.2016). The recruitment period was January 2017 to March 2019 and we planned to recruit 104 patients according to the sample size calculation described below. After informed consent, we enrolled a total of 36 patients undergoing aSCT at the University Hospital of Erlangen. Despite generally frequent inclusion of patients and high acceptance rates of 95%, the study was prematurely closed due to logistical challenges, including the departure of key study personnel (e.g., the primary acupuncturist and study nurse) and insufficient funds to continue recruitment beyond 36 patients. Inclusion criteria were age ≥ 18 years regardless of their hematological malignancies and their remission state before transplantation. Exclusion criteria were start of conditioning chemotherapy before inclusion, active participation in other clinical trials and clinical depression defined by a Hospital Anxiety and Depression Score Germany (HADS-D Score) of ≥ 11 and antidepressant drug treatment. At inclusion, patients were given the questionnaires of the first visit before knowing which group they were in to reduce the influence of potential disappointment into the first dataset.
Control group and blindingSince the interventions as a whole could not be placebo-controlled or blinded, the control group received treatment as usual undergoing allogeneic stem cell transplantation, which in our department includes periodical psycho-oncological guidance. Questionnaires and outcome parameters mentioned below were collected and documented by our GCP certified study center for both groups equally. Once randomized, patients in the control group were offered a free one-time consultation on CAM after the study period.
RandomizationThe random allocation sequence was generated in one block with a block size of 4 using randomization.com. The results were sealed in a non-see-through envelope that was randomly mixed within the block. After enrollment in the study, the study nurse was informed. An independent person that was assigned for the study then drew one of the letters, opened it, wrote it on a list with signature and date. The study nurse then wrote the date of the randomization and the result into the electronic documentation system (eCRF). Study participants that didn´t finish the study were not replaced.
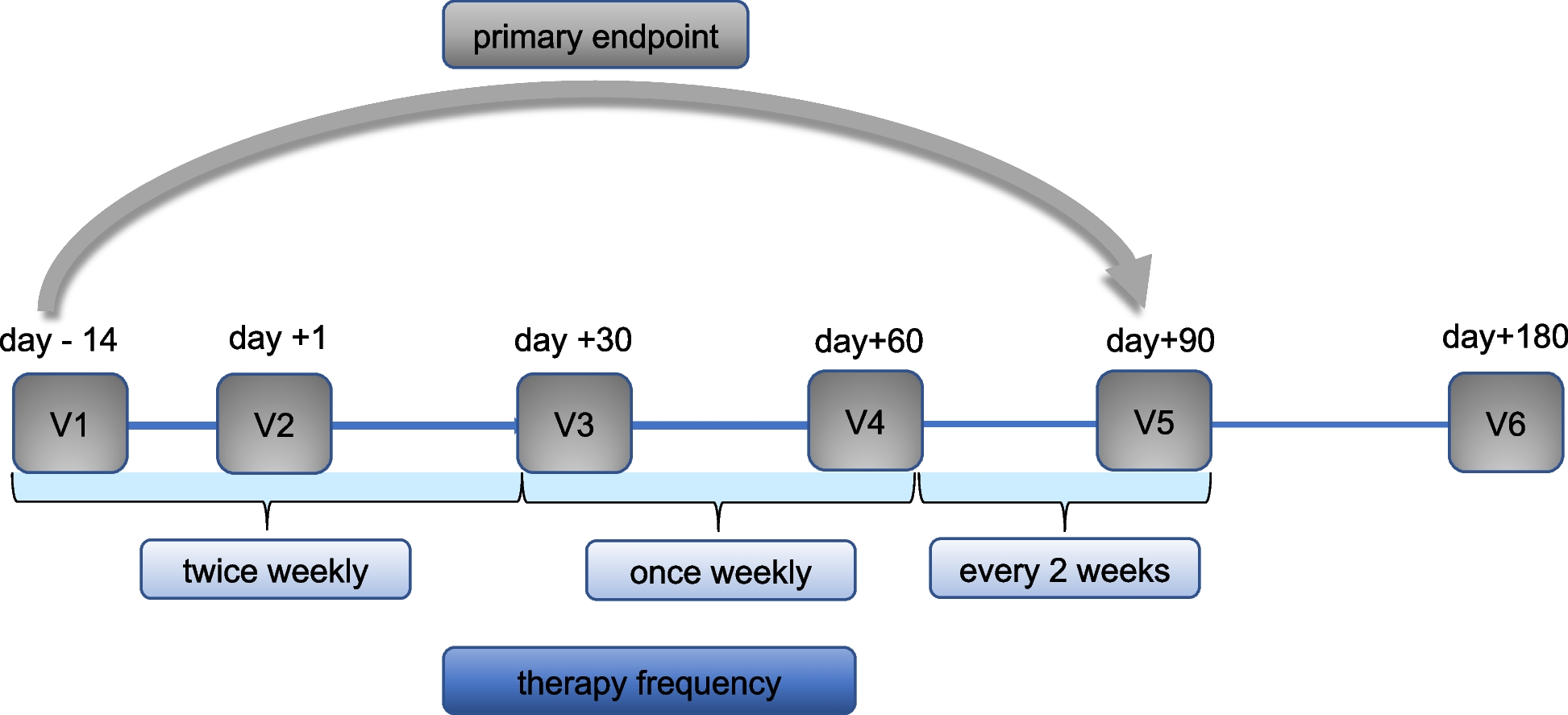
InterventionAll participants randomized in the intervention group were offered a multimodal therapy of complementary medicine always consisting of three methods e.g., TCMA, music therapy, and clown therapy between the visits at days −14, 0, 30, 60 and 90 as outlined in Fig. 1. TCMA was performed by a board-certified acupuncturist. TaKeTiNa sessions were led by a certified TaKeTiNa therapist. Clown therapy was conducted by a medical doctor trained in the Metzler method. Therapist-led interventions were delivered independently of each other and study visits. Each was scheduled twice weekly in the first month, weekly in the second, and biweekly in the third. Post-discharge, interventions aligned with study visits. Patients were advised to practice TaKeTiNa and clown exercises independently between sessions using a booklet, though frequency was unspecified and adherence was not monitored. There were no specific clinical criteria required for their application. The 10-min duration for TaKeTiNa and clown therapy was chosen based on our prior clinical experience (2014–2016) with individual aSCT patients, which indicated that shorter sessions were better tolerated amid treatment-related symptoms and fatigue while still reported as beneficial. TCMA: Patients were diagnosed according to TCM by a board-certified acupuncturist using the 5 elements, the 8 principles and pathogenic factors on each visit according to Kaptchuk 2002 [10]. Pulse and tongue diagnosis were performed at each visit. Before every acupuncture session, a brief assessment was made using the above diagnostic tools. Then, depending on the underlying current imbalance, 5 to 20 acupuncture points were selected. After skin disinfection, needles were inserted until a DeQi sensation (a feeling of spreading warmth or electric sensation) was reported by the patient. Needles with a 0.16 mm diameter and 15 mm length (Seirin® B type needle No.1, Japan) were used to minimize the risk of bleeding or infections. Unless discomfort was reported by the patient or a change in position was necessary, in which case the needles were removed, the needles remained for a total of 10–20 min before being removed. Patients with minor bleeding complications (e.g., small hematomas) remained eligible for TCMA, provided needles were not inserted into affected areas or sites with high bleeding or infection risk (e.g., thrombosis). No patients experienced severe bleeding complications that contraindicated acupuncture. Other than that, acupuncture was performed irrespective of fever, systemic inflammation, aGvHD, neutropenia or thrombocytopenia.
Fig. 1
Study design and trial profile. The figure shows the six clinical visits and their timeline (V1-V6). The intervention group received the multimodal therapy consisting of 20 min of TCMA and 10 min of each TaKeTiNa and Clown-therapy. The therapy was received twice weekly in the first month, then once weekly the 2nd month and once every two weeks for the 3rd month
TaKeTiNa music therapyDuring the first intervention, the principles of TaKeTiNa® were explained to the patient by a certified TaKeTiNa® therapist. Egg-shakers (NINOSET540®, Meinl, Germany) were used as percussion instruments. An additional booklet containing further instructions was given to the patients and they were encouraged to do exercises on their own in between the interventions (suppl. mat. 1: TriCAM Exercise Booklet) Then and in subsequent therapy-sessions lasting about 10 min, a one-on-one TaKeTiNa®-session was conducted laying, sitting or standing depending on the patients’ condition and preference using voice, feet, hands and optionally egg-shakers.
Metzler®-Clown-TherapyDuring the first intervention, the principles of Metzler-Clown-Therapy [9] were explained to the patient by a medical doctor with the necessary training. A clown nose was given to the patient as the smallest form of masquerading. Patients were encouraged to perform exercises from the booklet mentioned above on their own between the interventions. Then and in subsequent therapy-sessions lasting about 10 min, exercises were conducted laying, sitting or standing depending on the patients’ condition and preference using the 6 principles of relationship, roleplaying and archetypical characters (“Kellerkinder”).
Primary and secondary outcomesThe follow-up period for primary and all secondary outcomes was 6 months post-transplantation (visit 6). Data regarding the outcome parameters onset of GvHD, overall survival (OS), progression-free survival (PFS) and treatment related mortality (TRM) was assessed for up to 1 year of follow-up.
FACT-GThe Functional Assessment of Cancer Therapy (German version) was used to assess Qol. The primary endpoint of the study was the difference in the mean change of the FACT-G total score visit 5 compared to visit 1 between the groups.
Secondary endpoints: HADS-DTo evaluate the depression and anxiety of the patients, the Hospital Anxiety and Depression Score (German version; HADS-D) was used. A secondary endpoint was the mean change of the HADS-D depression and HADS-D anxiety score visit 5 compared to visit 1 between the groups.
FACT-G and HADS-D questionnaires were completed at each study visit (V1–V6) to assess QoL, depression, and anxiety over time, with the primary endpoint analysis focusing on the change from visit 1 to visit 5. Higher FACT-G scores indicate better QoL, while higher HADS-D scores reflect greater levels of anxiety or depression.
Safety of acupuncture in aSCTSince the patients were highly immunosuppressed and had temporary severe thrombocytopenia, we compared the cumulative incidence of soft-tissue-hematomas or soft-tissue-infections requiring treatment, defined as topical (e.g. band-aids) or systemic (e.g. antibiotics) between the groups from visit 1 to visit 5.
Other endpoints at month 3 (visit 5) included ECOG Performance Status, Karnofsky Performance Status, pneumonias, viral infections, hospitalization days, and stationary costs from visit 1 through visit 5 between the groups.
Statistical analysisDue to the lack of previous scientific data, we calculated the effect size of the primary outcome parameter after 5 patients of each group had been enrolled and had completed visit 5 using a two-sided Wilcoxon-Mann–Whitney test. From this estimated effect size, a target population of 104 patients was calculated. The analysis was planned as intention-to-treat (ITT), so that from visit 2 on, in case of a premature dropout before visit 5 (endpoint), the last documented visit was used as visit 5 for that patient. We planned prospectively to measure the differences in groups for endpoints FACT-G, HADS-D by performing a two-sided WMW-Test. To assess the development of FACT-G sum-score and subgroups over time (V1–V6), a linear mixed-effects model was used, the mixed effect ANOVA, which incorporates fixed effects for group (intervention vs. control), visit (time), and their interaction (group * visit) and a random effect for patients to account for repeated measures. The P-value for the group * visit interaction indicates whether the QoL trajectory differed between groups. As the found interaction was not significant, pairwise comparisons between groups were omitted. The survival probabilities (OS, PFS) and incidence of aGvHD were estimated by using the Kaplan‐Meier method and were compared using the log‐rank test. For other endpoints shown supp. table 1- 3, two-sided p-test was performed. If not otherwise stated, error bars in the graphs display the mean SD. The results were generated by Graphpad-Prism® version 9.1.2
Comments (0)