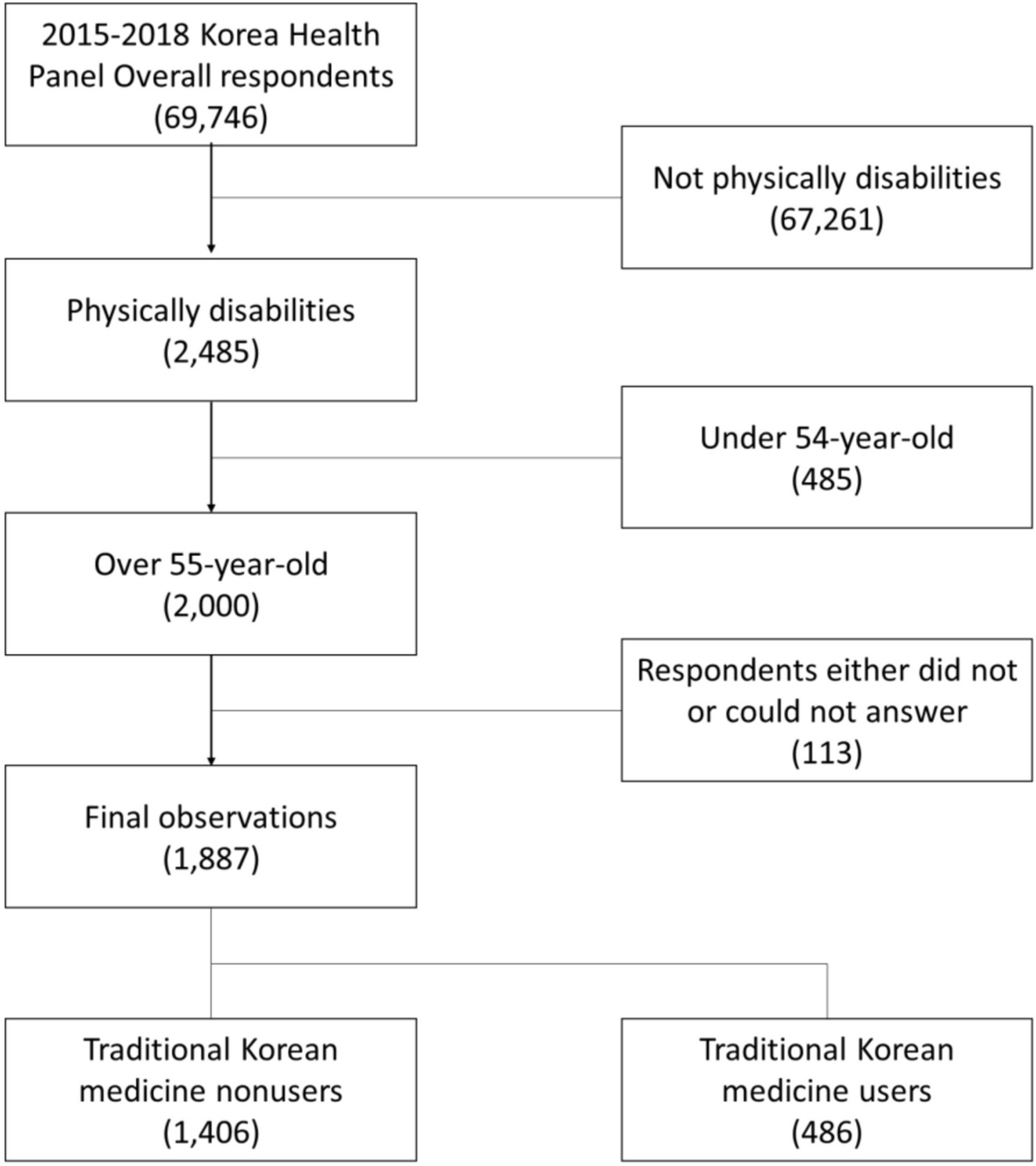
The current study used KHP data from 2015 to 2018 to analyze the status and expenses of TKM utilization and their influencing factors for individuals with physical disabilities through a panel analysis using logistic regression and panel hybrid regression. Out of the 1,887 observations, 486 (25.76%) utilized TKM. Females and individuals between 65 and 74 years of age, those with an education level of elementary school or less, individuals covered by NHI, those experiencing chronic musculoskeletal and neurological diseases, individuals with CCI of 1, and low ADL and IADL, and those without having neoplasm diseases were significantly associated with a higher rate of TKM utilization. In terms of expenses, females and individuals aged between 65 and 74 years, NHI holders, those who with chronic musculoskeletal or neurological diseases, without neoplasm diseases, and with a CCI of 1 had significantly higher medical expenses. When panel analysis using logistic regression was applied, females, those with chronic musculoskeletal diseases, CCI of 1, and with more chronic conditions had a higher percentage of the TKM utilization. When panel hybrid regression analysis was applied, females, NHI holders, patients with chronic musculoskeletal diseases and more chronic conditions had higher medical expenses.
Several international studies investigated the factors related to the T&CAM utilization. A study conducted in Europe reported that 10–40% of the population in each country utilized T&CAM, and health condition, sex, education, and income influenced the utilization of T&CAM [24]. According to the 2007 National Health Statistics Reports in the US [25], almost 40% of the population utilized T&CAM, while another study [26] mentioned that the T&CAM utilization was dependent on sex, age, education, marital status, income, insurance, location, physical activity, alcohol usage, smoking, and body mass index (BMI). Quan [27] investigated whether the American population had a positive perception of the T&CAM utilization and found that factors such as age, sex, ethnicity, cultural background, financial stability, education, health condition, and cost influenced the T&CAM utilization. In the case of Korea, Park [28] explained that sex, marital status, financial status, perceived health condition, and limited mobility due to pain were significant influencing factors of the TKM utilization.
According to studies on the T&CAM utilization by individuals with physical disabilities, Krauss [11] showed that the rate of the T&CAM utilization is higher than that of the general population, and that there is significant correlation between education and financial status and the T&CAM utilization. Whereas, there is no significant relation with ethnic identity, sex, and age, which contradicts the findings of the current study. However, the study states that individuals who use T&CAM have a high percentage of having chronic pain and depression, and those with pain, depression, anxiety, insomnia, and headache have a higher rate of the T&CAM utilization. This is consistent with the findings of the current study, in which individuals with chronic musculoskeletal disorders and more chronic conditions and whose CCI is 1 had a higher rate of the TKM utilization. In a Canadian study [12], the frequency of the T&CAM utilization by children with physical disabilities was examined. The results showed that those with low health-related quality of life (HRQOL), whose mothers were highly educated, and who identified themselves as Canadian had a higher rate of the T&CAM utilization Meanwhile, in a study by Carlson et al., the utilization of T&CAM was higher in females, people from the West coast or Midwest, and previous users of T&CAM [13]. In addition, those with pain, hypofunction, and low energy utilized T&CAM, which is consistent with the findings of the current study in terms of sex and treatment conditions.
Based on KHP data from 2008 to 2015, the TKM utilization rate of individuals with physical disabilities was 21.27%, surpassing the overall TKM utilization rate for disabilities which was 17.6% [10]. In the current study, which analyzed data from 2015 to 2018, the rate of TKM utilization among individuals with physical disabilities was 25.76%, indicating a 4.5% increase and demonstrating a growing trend. Compared to the 71% of the entire Korean population who have experienced TKM in their lifetime, the rate of TKM utilization among individuals with physical disabilities is relatively low [29]. In a study analyzing the utilization rate of TKM by people with disabilities using the 2015 KHP data, the utilization rate for people with disabilities was only 14.3% of that for people without disabilities [30]. However, according to the 2018 current status of medicine utilization by individuals with disabilities and the total population according to institutions, the utilization rate of TKM clinics and hospitals by individuals with disabilities was 7.7%, which was higher than that of the total population (7.1%), of which the utilization rate of individuals with physical disabilities was relatively high at 8.4%.
In the case of individuals with physical disabilities, females showed a higher utilization of TKM, indicating a different trend from previous studies where females with disabilities were observed to receive treatment less frequently than males [31, 32]. However, in the domestic and international studies on the utilization rate of TKM or T&CAM, females ranked higher [24,25,26, 28], which is consistent with the findings of this study. Moreover, in the case of Korea, while the average number of hospital visits and period of hospitalization were higher in males, the usage of outpatient clinics was higher in females, showing a different usage pattern according to medical service [33]. In other words, females use diverse medical services more frequently than males, and this trend is consistent in the population with physical disabilities.
This study conducted a panel analysis of the medical expenses for TKM, distinguishing between intra and inter-subject effects. The results showed that the intra-subject effect had statistically significant variables, and in the aspects of the type of medical area, the existence of chronic musculoskeletal disorder, and the number of chronic conditions only the inter-subject effect was statistically significant. The fact that there was no intra-subject effect indicates that changes in the individuals did not influence their TKM expenses. The factors that influenced TKM expenses changed only through their innate characteristics. For example, in research from 2015 to 2018, patients who had newly developed chronic musculoskeletal disorders showed no change in TKM expenses. However, those who already suffered from chronic musculoskeletal disorders prior to the study had higher TKM expenses than those who did not. This finding is consistent with that of other studies on TKM services, as one study that conducted a panel analysis on patients with cancer showed no intra-subject effect [34]. This could be understood as a feature of TKM utilization, where those who were using TKM continuously used it regardless of time, while those who did not seek TKM continued not to use it despite worsening health conditions.
In this study, the higher the number of patients with chronic musculoskeletal disorders or conditions, the higher the utilization rate and expense of TKM, which is consistent with the general characteristics of T&CAM utilization. According to a study by Park [28] on the first-year aging panel that took place in 2006, the utilization of TKM was markedly high in female, those with higher education status or lower income, those who were not married, those living outside of the city, and those who had limited mobility due to pain. As pain resulting in limited mobility is frequently caused by chronic musculoskeletal disorders, the utilization of TKM services by individuals without disabilities and those with physical disabilities is relatively similar. According to studies abroad, T&CAM is sought mostly for pain-causing disorders [9, 13].
The finding that the utilization of TKM services is high among patients with disabilities and chronic musculoskeletal disorders have several implications. The problems that persons with physical disabilities frequently suffer from are upper back pain, knee joint pain, and musculoskeletal disorders such as miscellaneous spine diseases are ranked high [35], which matches the disorders that patients seeking TKM suffer from [36]. Therefore, TKM can provide health management services to individuals with physical disabilities. At the same time, the closer the CCI is to 1, the higher the utilization rate for TKM, which indicates that individuals with physical disabilities without severe comorbidities frequently use TKM. This could be due to the lower percentage (19.5%) of those with severe disabilities among those with physical disabilities compared to 80.5% of those with less severe conditions [37]. However, the possibility that severely disabled persons could not use TKM due to low accessibility cannot be eliminated. In particular, the high TKM service expenses of NHI holders indicate that basic TKM services provided are limited. Expansion of the NHI coverage of TKM services is necessary in the future, as observed in a study by Park [28].
The current study had some limitations: First, due to the nature of the panel survey, KHP is likely to cause a selection bias. As the panel deviates over time, it reduces the representativeness of the entire Korean population. In addition, there is a possibility of an information bias that generates information inaccuracy because KHP is the survey that was conducted by individuals self-reported responses only using CAPI (Computer Assisted Personal Interviewing). Second, the total number of data observations was 1,887, and the total number of individuals with disabilities who used TKM services are 486. Therefore, if the participants were distributed according to each variable, each distribution would be low in number, which could reflect outliers. Third, while the total expense according to variable could be measured using panel hybrid regression analysis, the specific cost according to variable could not be interpreted because of the log substitution of the expense. Fourth, the lack of studies on T&CAM utilization by individuals with physical disabilities made it difficult to fully discuss the findings of this research. Fifth, the current study focused on the utilization of TKM, consisting of acupuncture, moxibustion, chuna, traditional Korean herbal medicine, etc.; Each country’s definition of what constitutes T&CAM is different; therefore, the findings cannot be generalized to other countries The findings of this study need to be interpreted based on each country’s medical policies and T&CAM status.
Despite these limitations, this study is meaningful in that it is the first analysis of TKM utilization among individuals with physical disabilities in Korea. In addition, the fact that this study resolved the endogenous problem caused by unobserved individual characteristics that could occur in a cross-sectional study by adopting a panel analysis on longitudinal data from four years, which is rare in T&CAM utilization studies, is meaningful in terms of methodology. Moreover, as it analyzed the influencing factors of the utilization and expense of TKM services in individuals with physical disabilities, it could be used as a foundational study to provide efficient TKM services to individuals with physical disabilities in the future and hopefully act as a cornerstone for legislation regarding the same.





Comments (0)