
Remember me




Nineteen medical herbalists participated in the study, with ages ranging from 24 to 57 years (mean = 35 years). The majority (n = 16, 84.2%) were males. The sex imbalance is consistent with the lower number of female medical herbalists practicing in Ghana compared to males. Nearly half (n = 9, 47.4%) practiced in integrated healthcare facilities, while the remainder operated in private THM clinics. All participants were general practitioners, treating various ailments including malaria. The coastal belt (Cape Coast) had the highest representation (n = 9, 47.4%) among participants (Table 1).
Table 1 Characteristics of study participants (N = 19)ThemesThematic analysis of participant narratives revealed five key themes (Table 2):
1.Benefits of THM Practice: This theme explored the perceived advantages of THM use.
2.Knowledge/Understanding of THM Integration: This theme examined participants’ understanding of the integrated healthcare model.
3.Structure/Infrastructure for Integrated Care Delivery: This theme addressed the physical resources and settings associated with integrated healthcare delivery.
4.Processes/Activities in Integrated Healthcare Delivery: This theme described the activities and workflows involved in the integrated care model.
5.Outcomes/Consequences of THM Integration on Malaria Control: This theme investigated the perceived impact of THM integration on malaria management in Ghana.
Benefits of THM practiceParticipants highlighted various advantages of THM practice, including its perceived efficacy, minimal side effects, and job creation potential. Participants believed THM offers faster malaria cures due to the body’s familiarity with such remedies. Others acknowledged that although all medications have side effects, those associated with THM were considered negligible. Additionally, some participants viewed the traditional health system as a source of employment, with private THM clinics creating job opportunities for the populace. The quotes that follow expatiate on the views expressed by participants regarding the merits of THM practice in Ghana:
Efficacy of THMI can say herbal medicine cures malaria better than orthodox medicine. Our human system knows herbal medicine. It is like introducing food to your baby…. Our system accepts herbal medicine well [Participant 12, Cape Coast].
Minimal side effectsAll medications have side effects. Once it is an external thing that you are introducing into your body, there will be some side effects. But it is up to the degree of the side effects. When you compare the side effects, it is less for herbal medicines than the orthodox medications [Participant 11, Cape Coast].
Employment creation…THM has created jobs in Ghana. For example, when you go to Kumasi, there are a lot of herbal clinics/outlets that have been established and these clinics have and keep employing people [Participant 1, Cape Coast].
Knowledge/understanding of the practice of integrated healthcareParticipants generally demonstrated awareness of THM integration into the Ghanaian healthcare system. They specifically mentioned the establishment of a Traditional Herbal Medicine program at KNUST as evidence of this integration.
I am aware of the integration. Perhaps, that is why they have started teaching THM at KNUST. We have students from ‘Tech’ that are studying THM as a course to become professionals [Participant 5, Cape Coast].
This suggests that participants perceive the inclusion of THM within the formal education system as a significant step towards its legitimisation and integration within mainstream healthcare delivery.
Structure/infrastructure associated with integrated healthcare deliveryThis theme addressed the physical resources and settings associated with integrated healthcare delivery. Four key sub-themes emerged:
Availability of integrated health facilitiesParticipants acknowledged the presence of THM units within some government hospitals. However, they expressed concern about the limited number of these facilities. They attributed this inadequacy to factors such as low public awareness, insufficient government support, and consequently, low patient utilisation of integrated healthcare services.
…we have 55 piloted facilities. That number is small compared to the number of orthodox healthcare facilities in the country. That also accounts for the unpopularity of the THM unit in the country because the more there are herbal medicine facilities, the more people will get to know and patronise such facilities [Participant 11, Cape Coast].
I am aware of the availability of integrated facilities. We have Tafo government hospital, Juaben government hospital, Bekwai, and in Accra we have LEKMA hospital, Police hospital, Tema general hospital, and then the Tamale teaching hospital, Ho government hospital, and Wawra government hospital in the Oti region. So, it is all over the country [Participant 14, Kumasi].
In the Upper West region, there is one there. That is, the Wa municipal hospital. There are about two medical herbalists at the Wa Municipal hospital [Participant 4, Wa].
Quality assuranceParticipants practicing within integrated health facilities highlighted their commitment to quality healthcare delivery. They described adhering to established medical principles and protocols for patient care which included prescribing only herbal products listed on the Ministry of Health’s recommended herbal medicine list. Additionally, some participants viewed regular inspections by the FDA as a means to ensure the quality, efficacy, and safety of the herbal products and services they provide.
We have the recommended herbal medicine list. So, the recommendation should be based on the list from the Ministry of Health which has been certified so we stick to defined medical principles [Participant 2, Wa].
These days, once you are a certified THM provider, the FDA will come for inspection and check that your facility is following scientific methods to ensure quality, effectiveness, and safety to those who would use it [Participant 6, Cape Coast].
Inadequate health personnelParticipants highlighted a shortage of qualified healthcare personnel within integrated healthcare facilities. They described performing multiple roles beyond their core duties, including procurement, reporting, medication request follow-up, and drug dispensing. This role overload was attributed to the limited number of staff and a perceived lack of personnel with expertise in herbal medicine. Furthermore, some participants suggested that existing medical herbalists might be drawn to other career paths, such as academia or positions with the Ghana FDA, potentially exacerbating the staffing shortage.
In our case, we must initiate, follow up with memo to request for medications. They say they don’t know much about herbal medicines, so I must take charge and lead the procurement. So, you become part of pharmacy because you have to monitor and make sure they are dispensing the right drugs. So you move up and down; it is a lot of work because one person you are involved in reporting, payment process, monitoring, and everything [Participant 2, Wa].
…comparing to the country’s population, I don’t think we have enough qualified medical herbalists. The whole of Cape Coast metropolis, we are just five. Can you imagine! [Participant 8, Cape Coast].
The numbers are not enough…. we started herbal medicine in KNUST in 2001 and most of us don’t practice. They enter a different sector like FDA. Those who really practice is very few. They just branch into a different field. Some are in academia and the FDA [Participant 17, Kumasi].
Insufficient medicines and equipmentThis sub-theme emerged primarily among participants from the forest belt. They reported experiencing disruptions in service delivery due to a shortage of essential herbal medicines. They attributed this shortage to cumbersome procurement processes perceived as overly bureaucratic. Additionally, delays in deliveries from approved manufacturing centres were identified as contributing to stockouts. These shortages reportedly hampered their ability to provide quality care.
In contrast, participants from the coastal belt highlighted the issue of inadequate equipment, particularly a lack of computers. This lack of technology was perceived as hindering their productivity and overall job satisfaction. They associated this equipment deficiency with limited or absent funding for integrated healthcare facilities.
We sometimes run out of drugs because to order the drugs must pass through so many bureaucratic lines. When I talk about the bureaucratic system, I mean that it must go through many offices before it gets approved. Over here, they will bring the pro forma invoice then we work on it and get the voucher from the account. Then the signatory must come from different people. So, if one signatory has travelled, it becomes a challenge to order the drugs, hence limited or no drugs [Participant 16, Kumasi].
When we order our medicines from Akuapem Mampong, it takes a long time. It delays and that doesn’t help because the client needs it, which disturbs you too. Why should you delay in giving treatment to someone suffering from malaria? [Participant 15, Kumasi].
… We don’t have computers to assist with our work. And today, everything is e-health and so, if I do not come with my personal computer, then it means that I will be unable to work. Computer is a basic equipment that we think if we had, it would improve our healthcare delivery, but we don’t have them due to the lack of funds. It doesn’t make the work enjoyable [Participant 8, Cape Coast].
Processes/activities related to the delivery of integrated health servicesThe main issues identified under this theme were categorised into five sub-themes; health system-based challenges, national/general challenges, patient-centred care, follow ups, and THM training and research.
Health system-based challengesThis section explores challenges identified by participants within the processes and activities related to integrated healthcare delivery for malaria control. Two issues emerged: First, disapproval from orthodox medicine providers: Participants expressed concerns regarding negative perceptions and attitudes towards THM integration from some orthodox medicine providers. These negative views were perceived to hinder effective collaboration and patient referrals. One example cited by participants was the misconception that THM can cause kidney and lung problems. They reported efforts to address these misconceptions through clinical meetings, but with limited success.
Another challenge we are facing, which we are trying to solve has to do with the attitudes and perceptions of the medical doctors and other orthodox practitioners. They have the perception that when you take herbal medicine, it will affect your kidneys and lung. it is a major challenge to the integration. We organise clinical meetings to explain to them, yet they are not convinced [Participant 8, Cape Coast].
……for the medical doctors, they don’t want to hear about THM. They think that they go to school to learn about scientific medicine. But they don’t know that currently THM providers also go through scientific training. Their opposition is one of our challenges [Participant 3, Wa].
Secondly, participants, particularly those from the coastal and savannah regions, highlighted challenges associated with referral practices within the integrated healthcare system. They reported that orthodox medical doctors often exhibited reluctance to formally refer patients to medical herbalists. Instead, some doctors resorted to informal methods of recommending THM, blurring the lines between a formal referral and casual advice.
Participants attributed this reluctance to several factors:
Perceived Superiority: Some medical herbalists believed that orthodox doctors held a sense of superiority, viewing them as apprentices rather than qualified healthcare providers.
Patient Affordability Concerns: Participants suggested that doctors might hesitate due to concerns about patients’ ability to afford certified herbal medicines offered at integrated facilities, as these often require out-of-pocket payments.
It is difficult for the orthodox medicine provider to accept and refer patients to us. For those who refer, they do it ‘backdoor’, in the form of an advice rather than as a formal referral [Participant 6, Cape Coast].
…the medical doctors prefer to treat malaria cases rather than referring to us…like I said, the herbal medications are cash-and-carry. So, the doctors are concerned about the cash. They are not certain that the patient will pay for the medication, and so, they prefer to treat the patient with their medication rather than referring them for herbal treatment [Participant 8, Cape Coast].
For my practice over ten years, no medical officer has referred a patient to me. We have a referral form that we fill. The challenge is that they frown on our referral forms. So, what we do is to refer the person verbally…. we do it in an informal setting. we don’t have a problem referring patients to the orthodox. But they will not do that. Why will they [orthodox] do that? They see themselves as superior, so why would they want to refer to us? They [orthodox providers] see us as apprentice. [Participant 19, Wa].
National/general challengesThis theme highlighted issues at the national level that hindered effective management of malaria through the practice of integrated healthcare. Major national/general challenges that emerged were non-exhaustive NHIS coverage and inadequate promotional activities on THM integration. Participants narrated that the non-comprehensive nature of the NHIS (exclusion of herbal anti-malarial drugs) accounts for low patronage of services at THM clinics at integrated hospitals because clients always opt for free orthodox anti-malaria medicines rather than paying full cost for the herbal ones.
…. the malaria medication for orthodox is on the health insurance but when you opt for the herbal medicine, then you will be paying about ghs80 or more. So, free or ghs80? The cost involved is what is accounting for the low patronage of herbal medicines for malaria in our THM clinics [Participant 18, Kumasi].
Promotional activities play a vital role in the successful implementation of interventions. When the providers were asked to share their experiences concerning publicity of integration and its implication on malaria control, they gave an account, which suggests inadequacy of promotional activities regarding the integration programme.
… One major challenge we are facing with this integration is the lack of publicity or awareness. Most people don’t know about this integration. The Ministry of Health should have projected the integration right from the onset. Now, when you visit these selected hospitals (integrated facilities), there are herbal practitioners available, but people do not know about that, so they do not patronise our services [Participant 8, Cape Coast].
Patient-centred careWhen discussing patient care, participants recounted that attending to their clients on time and spending ample time with them is something they were proud of. They emphasised that the patients really appreciated that kind of care unlike the orthodox unit, where less time is spent. The ensuing quote represent this finding:
It is something we are very proud of at our unit. We spend a lot of time, about an hour with one patient.…. They really do appreciate that unlike the orthodox side that within 2–3 minutes they are done and don’t have time for them. So, when it comes to patient-provider relationship, it is the best in our unit [Participant 11, Cape Coast].
Follow upsWe found that follow ups, which is a feature of functional health systems was well implemented by the participants. They narrated that their desire to promote the welfare of clients motivated them to follow up and conduct medical reviews to avert undesirable treatment outcomes.
If you are interested in a case, then you follow up! There are others (clients) that I had to give my contact for them to call back. I do this to avoid any adverse effect of the treatment or medication [Participant 2, Wa].
… Some of the clients come for review. Through the follow ups we schedule reviews. After taking the THM, we don’t let them stay home. We schedule reviews and when they come, we test and make sure they are fine [Participant 15, Kumasi].
We also do a lot of follow up on our patients. We call to check up on them and find out whether they have had any side effects [Participant 8, Cape Coast].
THM training and researchParticipants recognised that the practice of integration has boosted research on herbal remedies for treating malaria. They perceived the herbal anti-malarial medications prescribed and utilised within the integrated system to be safe and effective because they go through scientific scrutiny at the Centre for Research into Plant Medicine and/or the Nogouchi Memorial Institute for Medical Research. The quotes below reiterate this finding:
I think it has boosted research on THM for malaria control because herbal anti-malaria drugs must be tested either at Nogouchi Memorial Institute for Medical Research or Centre for Research into Plant Medicine to verify whether it is safe for human consumption [Participant 1, Cape Coast].
Our THM comes from the Centre for Research into Plant Medicine; a lot of research has gone into these products, and they are safe for use. They are now safe and efficacious for treating malaria [Participant 15, Kumasi].
In addition, participants within the forest belt reported that they usually undergo continuous professional development training. According to them, such trainings were organised by the traditional and alternative medicine directorate and involved the interpretation of scientific medical activities such as x-ray reading, understanding laboratory results and clinical emergencies. They believed that this knowledge enabled them to interpret and confirm diagnosis of diseases, especially malaria. The quotations below summarise this report:
…. as medical herbalists we go for continuous professional development training. The training is mostly dependent on current situations. So, if there is a new herbal medication or new ways of doing things, we do that to improve upon the knowledge that we have. If there are research works going on, they update us on findings. We also do research because science is always updating. The training is mostly done by the Traditional and Alternative Medicine Directorate. They organise and get resource people to take us through it [Participant 14, Kumasi].
We have been going for continuous professional development (CPD) training. We do it yearly to upgrade our practice and the training largely depends on the topics that we deal with in that year. We have received training on the interpretation of x-rays, lab results and clinical emergencies…. the knowledge acquired enable us to request for lab testing and interpret the results to confirm our diagnosis for malaria [Participant 15, Kumasi].
Interestingly, participants at the savannah belt believed that THM training focuses on exposing medical herbalists to both modern/orthodox and traditional medicines. However, the same could not be said for orthodox medicine providers where training is more focused on orthodox approaches. This unbalanced training was perceived to have created knowledge gaps among mainstream healthcare providers, leading to a lack of understanding and appreciation of the contribution of THM to healthcare delivery in Ghana.
Some of the orthodox practitioners do not understand herbal medicine. We are trained to understand both orthodox and herbal medicines, but they are not trained that way. We have an appreciation of both sides but for them, they weren’t trained like that. They were trained one-sided and so they don’t understand herbal medicine, creating opposition from them [Participant 2, Wa].
Outcome/consequence of the practice of THM integration on malaria controlA key aspect of the study was to explore the perceived impact of THM integration on malaria control. Participants identified two main impacts - reduced pressure/burden on orthodox medicine providers and evidence-based THM practice leading to appropriate management of malaria. The participants perceived that their presence at public hospitals reduced pressure on orthodox medical doctors because they mostly treat malaria cases at their units and that the majority of the clients prefer herbal anti-malaria medication such as the ‘Mebeema’.
When you take the cases we treat in our unit, malaria is among the top five. So, if the orthodox doctor was treating about 1,000 cases, the numbers have reduced now because most people want to use the herbal anti malaria medicine, that is, Mebeema [Participant 11, Cape Coast].
…. even in our facility, we have about three different drugs for malaria. The most potent one is Mebeema from Akuapem Mampong. It has been used in the system for long and the response has been very good. Lots of people who come to the unit opt for it. Clearly, our presence here at the hospital has reduced pressure on the orthodox providers [Participant 16, Kumasi].
Besides, reducing pressure on orthodox medical doctors, participants irrespective of location, reported that the integration of THM has been beneficial because malaria cases are now appropriately treated through the evidence-based practice of their field. They believed the application of scientific clinical procedures such as correct diagnosis through laboratory testing/prescription, health education, and FDA approval of herbal anti malarial medications have led to effective malaria treatment, hence reducing prevalence. The following quotes elaborate on the views expressed by the study participants.
I will say that about 50% of our clients come for malaria treatment. Just as they do for orthodox medicine, we also make sure that the client is taken through education, then we ask them to get tested through the lab and confirm they have malaria before we allow them to take our medication. Evidently, we apply scientific clinical procedures in treating our clients, and it has proven effective because the cases are reducing, and people are getting healed quickly [Participant 9, Cape Coast].
… integration has helped. …. At first, they will go to the market and get anything. But now, they (patients) come to the hospital and go through the process before receiving treatment. Malaria cases have gone down in recent times. When they come in for the medication, we also advise them to keep their environment clean and sleep under treated bed net. So, it is difficult for you to see someone come here with malaria, get treated and return to the hospital again because of malaria [Participant 14, Kumasi].
…. integration has helped a lot in controlling malaria in the country. I say that because the medicine has gone through FDA to be tested for its effectiveness and safety. If the patient takes the medications according to the prescription, you realise that most of them recover fully due to our medication. Many times, we are able to even treat severe malaria, so the cases are reducing [Participant 13, Wa].
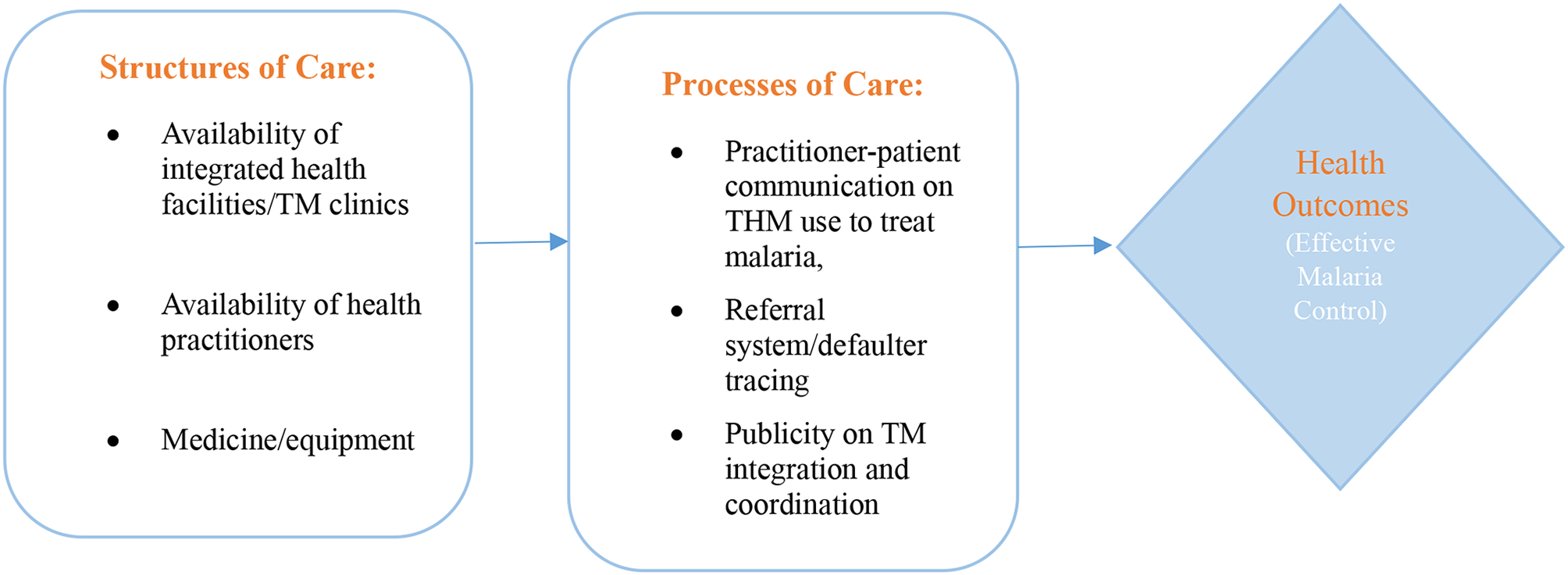
Figure 3 summarises the study findings guided by Donabedian framework for evaluating quality healthcare. Findings relating to infrastructure have been placed under the ‘structure’ component of the framework, while issues/activities that involved direct health service delivery have been grouped under the ‘process’ component. The effect of structure and process are presented under ‘outcome’ (Fig. 3).
Fig. 3
Summary of study findings guided by the framework for evaluating quality of healthcare
Comments (0)