
Remember me
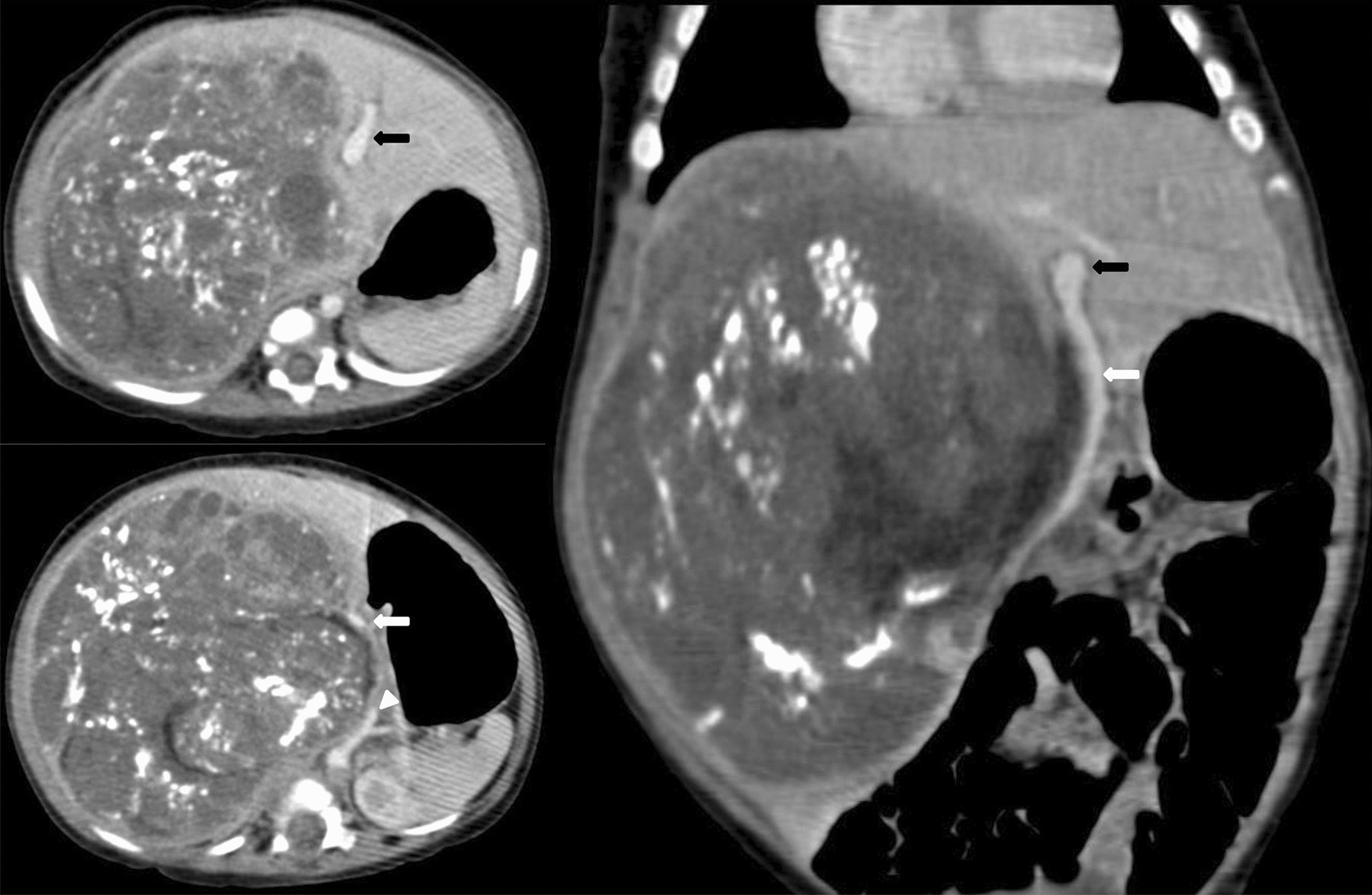

An 8-month-old child presented with an abdominal lump that had been present for the past month. A contrast-enhanced computed tomography (CECT) scan revealed massive hepatomegaly, with a 10.9 × 10.8 × 13.3 cm heterogeneously enhancing mass occupying the entire right lobe and the caudate lobe of the liver (Fig. 1). The mass showed extensive chunky calcifications, as well as necrotic and cystic hypodense areas. The inferior exophytic component displaced the portal structures anteriorly with splaying of the hepatic arteries and non-visualization of the right branch of portal veins. The aorta, celiac artery, and superior mesenteric artery were displaced along the medial border of the lesion, while the inferior vena cava (IVC) was compressed and not visible. Adjacent organs, including the gall bladder, kidney, and adrenal gland, were severely compressed and displaced. The alpha-fetoprotein (AFP) level was elevated to 860,000 ng/mL. Based on the radiological extent of the disease, the patient was categorized as having PRETEXT III disease with an annotation factor V + (venous) and stratified as having high-risk hepatoblastoma. The patient received seven cycles of SUPERPLADO regimen chemotherapy, which consisted of doxorubicin and alternating cycles of cisplatin and carboplatin over a period of 13 weeks. A follow-up CECT showed stable anatomical disease and a satisfactory biochemical response, with the AFP levels dropping to 171 ng/mL. A right extended hepatectomy was planned following a multidisciplinary meeting.
Fig. 1
Post chemotherapy contrast-enhanced triphasic computed tomography, showing heterogeneously enhancing lesion with chunky calcification and necrotic non-enhancing spaces involving the entire right lobe with a large inferior exophytic component. The portal structures, aorta, and adjacent organs are grossly displaced by the mass. The main (white arrows), left branch of portal vein (black arrows), and common hepatic artery (arrow head) are stretched anteriorly along their medial edges while the right branch and inferior vena cava are not visible due to compression by the lesion
A liver volumetry analysis conducted using Myrian software indicated a future liver remnant (FLR) of 72%. During the operation, the portal structures were not clearly defined, and the common hepatic duct appeared to be directly entering the liver mass. The right hepatic artery and the right branch of the portal vein were carefully dissected, looped, and divided flush with their entry into the mass. After the division of the right portal vein, the right hepatic duct was visualized. The hepatic duct confluence and the left hepatic duct were obscured and appeared flush, lacking clear demarcation on the under surface of segment 4b (Fig. 2). At this point, the right hepatic duct was cut close to where it entered the mass. The distal end of the right hepatic duct was cannulated using a 20-gauge epidural catheter. This stented duct served as a guide for the careful dissection of the left hepatic duct away from the liver lesion toward the left lateral sector. Tributaries from segment 4b were identified, ligated, and secured along this pathway. The main portal vein, appearing to continue as the left portal vein, was observed obscured in the umbilical fissure. It was gently dissected away from the under surface of the tumor. After achieving control over all inflow, a right extended hepatectomy was performed. Post-resection, an intraoperative cholangiogram revealed the left duct without any extravasation of contrast. The opening of the right duct was then ligated and secured. Hemostasis was confirmed, and the abdomen was closed with a drain placed in the surgical bed. Blood loss during the procedure was 300 mL. This report emphasizes the effectiveness of simple techniques, such as hepatic duct cannulation, to guide dissection and prevent inadvertent injuries, which could have necessitated a hepaticojejunostomy.
Fig. 2
a The liver delivered outside the abdomen after complete mobilization; b the proximal and distal stumps of the right portal vein (arrow heads) and hepatic duct (circled) while the left portal vein is seen stretched and displaced by the underlying mass. The proximal stump of the right duct is cannulated using a 20-gauge epidural catheter as a tactile guide to dissect the left duct safely. c Intraoperative cholangiogram after right extended hepatectomy showing the duct draining the segments 2 and 3
Comments (0)