In the current literature, there are still few studies that directly compare the outcomes of conventional titanium mesh (TM) and customized titanium mesh (CTM) in guided bone regeneration procedures. One of the most recent systematic reviews on this topic was conducted by Zhou et al., who performed a meta-analysis focusing mainly on the exposure rates between the two types of mesh. Their results showed a lower exposure rate for CTM (31%) compared to TM (51%). However, this review presents certain limitations. Most of the included studies were retrospective, with only one randomized controlled trial, and the analysis was centred only on exposure rates, without taking into account other important clinical outcomes such as vertical or horizontal bone gain, implant success or postoperative complications. Therefore a more comprehensive review is still necessary, besides exposure rates, also looks at other key clinical outcomes like bone gain and implant success, which are crucial for everyday clinical practice [35].
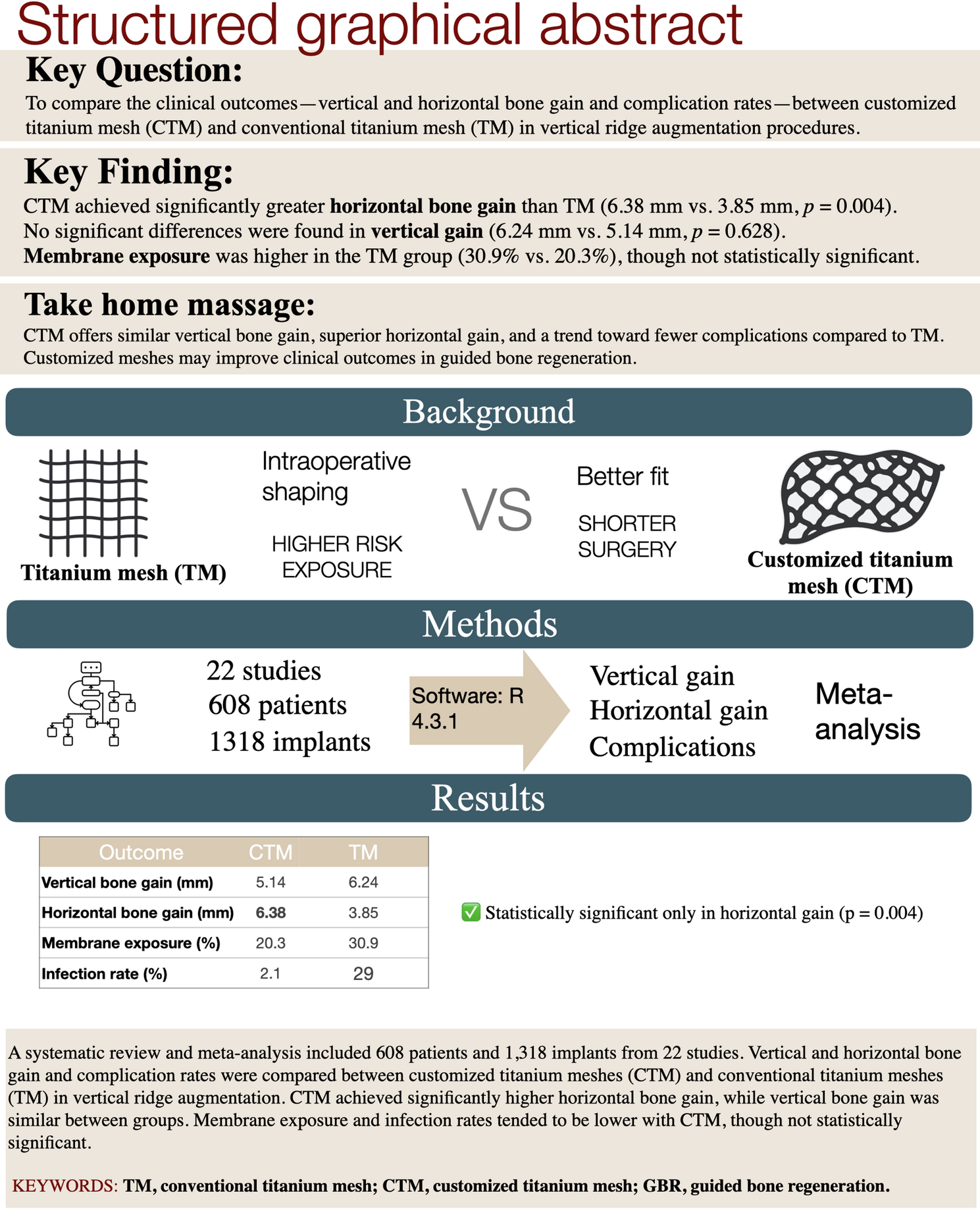
The primary objective of the present study was to assess and analyze the outcomes associated with both TM and CTM by reviewing the available literature and comparing their clinical performance. The findings indicated that the CTM technique demonstrated greater horizontal bone gain in comparison to the TM group. Regarding vertical bone gain, no statistically significant differences were found between the two groups. Although there was a noticeable tendency for fewer complications in the CTM group, this difference did not reach statistical significance, both in terms of membrane exposure rates and other complications, such as infections and dehiscences.
In this study, the mean vertical bone gain across groups was 5.65 mm, and the horizontal gain was 5.20 mm. These values seem to be higher than those reported by Sabri et al., who recently published a systematic review and meta-analysis focused on bone gain outcomes with titanium mesh. They found a mean vertical gain of 3.36 mm and a horizontal gain of 3.26 mm, although there was some variability among the included studies [36]. Unlike Zhou et al., who mainly focused on exposure rates, Sabri’s study looked at bone gain and also compared titanium mesh to other membranes like collagen. Still, it didn’t include a direct comparison between conventional and customized titanium meshes. In fact, only two of the 22 studies in their review evaluated results with customized titanium mesh, so the available evidence on that is still quite limited [35, 36].
In terms of vertical bone gain, the mean gain observed in the CTM group was 5.14 ± 0.38 mm. On the other hand, in the TM group, the mean vertical bone gain was 6.24 ± 1.51 mm. However, this value exhibited considerable variability across the included studies. For instance, the study conducted by Louis et al. reported a notably higher mean vertical gain of 13.5 ± 1.7 mm, while Torres et al. observed a considerably lower gain of only 3.3 ± 0.2 mm [21, 25]. Such discrepancies could likely be attributed to multiple factors, including differences in defect types (e.g., wide defects vs. narrow defects), measurement techniques (e.g., radiographic vs. clinical measurements) or surgical protocols (e.g., use of fixation devices, barrier membranes, or simultaneous implant placement). These variations highlight the complexity involved in interpreting vertical bone gain outcomes and emphasize the need for standardized protocols in future studies.
Regarding horizontal bone gain, the results showed a mean gain of 6.38 ± 0.60 mm in the CTM group. These results are consistent with the findings of Chiapiasco et al., who reported a mean horizontal gain of 6.35 ± 2.10 mm, suggesting comparable outcomes between both investigations [17]. Conversely, Pellegrino et al. observed a significantly greater mean horizontal gain of 9.3 mm [30]. This substantial discrepancy could be attributed to differences in defect size (larger defects may require greater regenerative volumes), graft volume (a higher volume may promote greater horizontal bone gain) or surgical techniques (variations in flap design, graft fixation, or membrane application) In the TM group, the mean horizontal gain was 3.85 ± 0.08 mm, a result that differs notably from the findings reported by El Chaar et al. in that retrospective study involving 39 patients, a higher mean horizontal gain of 6.42 mm was reported. This inconsistency may reflect differences in defect characteristics, patient selection, or surgical expertise [20]. The superior horizontal gain observed in the CTM group may be attributed to the customized mesh design, which allows for improved adaptation to the unique morphology of each defect, enhanced fixation, and superior stability of both the mesh and the graft material. Furthermore, titanium mesh produced through the 3D printing selective laser melting method exhibits robust mechanical properties and a smooth surface [35, 37].
It should be acknowledged that the observed difference in horizontal bone gain between CTM and TM may be influenced by anatomical heterogeneity among the included studies. Specifically, several studies involving CTM focused on posterior defects, particularly in the molar region, where larger horizontal augmentation is often required. In contrast, TM was frequently applied in anterior sites, where the morphology of the defect may limit the achievable horizontal gain. This distribution bias could partially explain the significant difference in horizontal bone gain observed in favor of CTM. Unfortunately, most of the included studies did not provide a detailed stratification of results according to defect location, limiting the possibility of subgroup analysis. Future studies should control for anatomical site to more accurately assess the impact of mesh type on bone gain.
The reported overall exposure rate was 25.3%, with 30.9% in the TM group and 20.3% in the CTM group. Although the CTM group exhibited a lower incidence of membrane exposure, this difference was not statistically significant. These findings align with those reported by Gu et al., who described a mean exposure rate of 22.7%, with 19.9% in the TM group and 25.2% in the CTM group [38]. On the contrary, Zhou et al. reported significantly higher exposure rates, with an overall exposure rate of 43%, including 51% in the TM group and 31% in the CTM group [35]. This notable difference may be attributed to disparities in sample sizes (608 patients in the present study vs. 247 patients in Zhou’s study) or greater heterogeneity in the study populations and surgical protocols.
Beyond membrane exposure, other complications such as dehiscence, partial or total graft loss, necrosis and abscess formation were observed. These complications were recorded in 29.8% ± 11.3 of cases in the TM group and 2.1% ± 1.7 in the CTM group. While this difference appears substantial, it was not statistically significant. Consistent with the overall exposure rate found in the conventional group (30.9%), individual studies such as those by Gomes et al. [31] and Poli et al. [32] also reported relatively high rates of membrane exposure, reinforcing the clinical relevance of this complication in non-customized protocols. In line with the general exposure rate found in the CAD/CAM group (20.3%), Jung et al. [34] reported titanium mesh exposure in 2 out of 10 patients (20%), despite the use of preformed, customized meshes. The authors emphasized that although minor exposures occurred, bone regeneration and implant stability were not compromised.
In a separate analysis, Urban et al. conducted a systematic review and meta-analysis comparing the effectiveness of different VRA techniques and their associated complications [39]. Their results showed that osteogenic distraction achieved the greatest vertical bone gain, with an average of 8.04 mm, followed by the inlay block technique, which had a mean gain of 3.46 mm. Urban’s study also examined the GBR technique, incorporating both non-resorbable and resorbable membranes, as well as titanium mesh. The mean vertical bone gain achieved with GBR was 4.18 mm. While osteogenic distraction provided the highest vertical gain, it also showed the highest complication rate at 47.3%, nearly double the rate observed for titanium mesh in the present study. Both Urban et al. and Alotaibi et al. reported comparable results, with customized titanium mesh achieving a mean vertical gain of 5.2 mm [7]. Both studies concluded that while osteogenic distraction achieved the greatest bone gain, it was also linked to the highest complication rate. Conversely, the GBR technique emerged as the most balanced approach, providing satisfactory bone gain with a lower risk of complications. Another study reported a premature exposure rate of 25.7% for d-PTFE membranes [40].
The exclusion criteria for this study required a minimum follow-up period of six months and a sample size of at least 10 patients, which may have excluded relevant studies. Furthermore, there was no standardization in the measurement methods, and the included studies provided limited data on the shape and size of the treated defects. These factors may have introduced bias in the results. Considering these limitations is crucial when making clinical decisions. Future studies should focus on conducting well-designed randomized controlled trials with larger sample sizes, extended follow-up periods, and standardized defect characteristics to further validate these findings.
The results of this review suggest that customized titanium meshes (CTM) may offer clinical advantages over conventional meshes, particularly regarding surgical handling and horizontal bone gain. The individual adaptation of the mesh facilitates easier contouring and soft tissue closure, potentially reducing the risk of complications such as infection or dehiscence. Although no significant differences were found in vertical bone gain or membrane exposure, the greater predictability in horizontal outcomes may be especially beneficial in cases requiring precise contour or volume. These findings may help guide clinicians in selecting the most appropriate technique for vertical ridge augmentation procedures.






Comments (0)