
Remember me
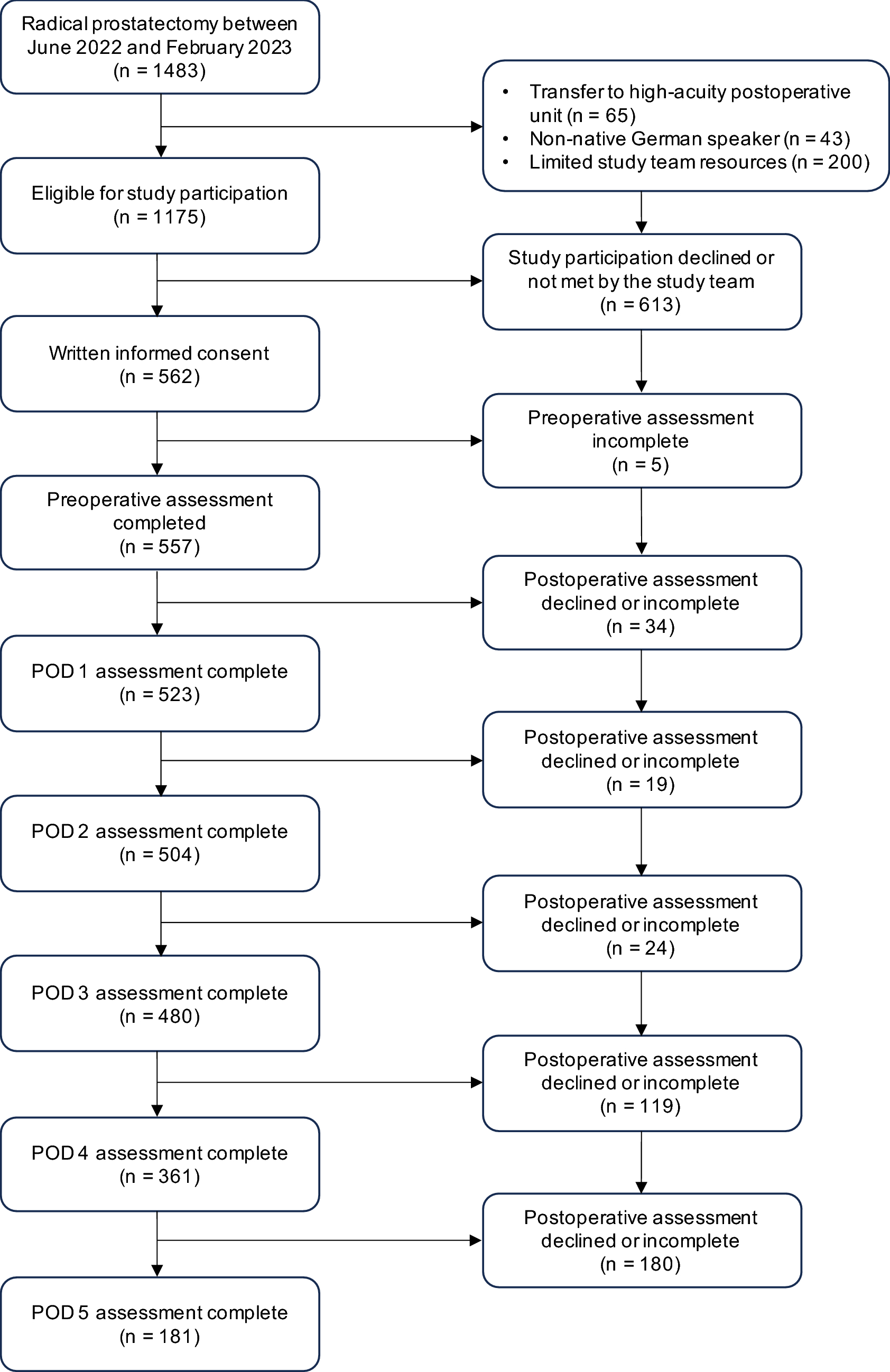
From the total number of 6,286 individuals who began the survey, 915 did not complete it, resulting in 5,371 completed responses. This group consisted of 2,082 participants from Australia, 1,280 from Ireland, and 2,009 from the UK. The median completion time for this survey was 14.0 min in Australia, 11.2 min in Ireland and 13.0 min in the UK. For our analysis, we used data from the 5,371 respondents who completed the full survey as there was no significant difference in MNL estimates before and after excluding respondents who spent less than 40% of the median completion time and consistently selected the same response for all questions (Appendix 2, Table 1 in supplementary materials; all models included in the sensitivity analysis are available upon request).
Table 2 provides the demographic characteristics of the analysed respondents from each country. Notable demographic differences included Ireland’s younger, more employed population compared to Australia and UK’s older, more retired respondents. Irish respondents also showed higher rates of religious involvement, multilingualism, and better self-reported health (except anxiety/depression). UK and Australian respondents had lower educational attainment and reported more health issues, though UK participants reported less anxiety/depression (Table 2).
Table 2 Socio-demographic characteristics of respondents from each countryComparison with national statistics showed a higher proportion of younger adults (aged 18–34) and a lower proportion of older adults (aged 75 and above) in the study sample compared to the general populations in Australia, Ireland, and the UK. The gender distribution was similar to national figures, with approximately half of respondents identifying as female in each country. Other characteristics, such as marital status, employment, and education, were broadly comparable to national profiles, though the proportion with a university degree was somewhat higher in the sample.
The impact of context on the EQ-5D-5L health states valuesResults from MNL models with interactionsAppendix 3 in the supplementary materials detail results from a range of MNL models with interaction terms which were estimated to examine how life expectancy (3-month versus 2-year), support level (limited and adequate), and varying combinations of life expectancy and support levels, affected health state values. Overall, the available level of support and the duration of life expectancy had a consistent statistically significant influence only on the death attribute. Although there were some significant interactions between the EQ-5D-5L coefficients, no consistent pattern was observed.
Appendix 3 Tables 1a-c show the impact of life expectancy on the valuation of health states. The results suggest that the influence of life expectancy was most pronounced in the UK sample compared to those in Australia and Ireland. In the UK, both 3-month and 2-year life expectancy scenarios had a significant impact on the death coefficient.
Appendix 3 Tables 2a-c present the impact of support level on health state values. The interaction between limited support and the death attribute was statistically significant across Australia, the UK and Ireland, whereas the interaction with adequate support was not significant.
Subsequently, the impact of each of the four contexts was examined individually, as documented in Appendix 3 Tables 3a-c. Table 3a findings show that in the Australian sample, only the worst-case scenario—3-month life expectancy with limited support—significantly impacted the death attribute, indicating a critical shift in death perception under these conditions. The other three vignettes did not show significant effects. Table 3b shows that only the interaction between a 2-year life expectancy with limited support context and the death attribute was statistically significant in the Irish sample. Spending two years in an environment with insufficient support may be perceived as prolonged suffering, making death seem preferable to continued life under such conditions. As shown in Table 3c, among the UK respondents, the 3-month life expectancy with limited support vignette was also significant. Additionally, the interaction term between context and no context in the 3-month life expectancy with adequate support vignette was significant. This indicates that the duration of life expectancy plays a crucial role in shaping how death is valued in the UK sample.
Finally, Table 3 provides results for each study arm to investigate the impact of contextual vignette information on health state valuation in the Irish sample (Australian and UK data presented in Appendix 3, Tables 4a-b the supplementary materials). The interaction analysis between health states and contextual scenarios revealed minimal systematic effects. Notable significant interactions included death health state in study arm 1 for Australia (0.483, p = 0.006), mobility levels MO2 and MO3 in study arms 3 and 4 respectively for Ireland (0.237, p = 0.032; −0.262, p = 0.007), and MO5 in study arm 2 for the UK (0.429, p = 0.013). While the magnitude of coefficients varied across countries, the pattern of effects remained relatively consistent. Model fit statistics indicated better performance in study arms 3 and 4 across all countries (Log-likelihood ranges: UK: -8616 to -9288; Australian: -9488 to -10,285; Irish: -5846 to -6154).
Table 3 Separate MNLs with main effects and interactions between a dummy indicating a vignette with or without a context and each attribute level for each study arm in the Irish sampleResults from separate MNL modelsSeparate MNL models1 were fitted for the context DCE and the no context DCE across each of the four study arms (defined by the context vignette) across each country. The magnitude of the coefficients within each dimension should increase reflecting greater deviations from the baseline as the severity of levels increases. Most of the coefficients were ordered as expected. To address nonmonotonicity in the dimension levels, we examined the coefficient estimates. Some levels showed unexpected patterns (either reversed ordering or inconsistent magnitudes compared to what theory would predict). To improve interpretability while maintaining model validity, we constrained these nonmonotonic coefficients to have the same value, effectively combining levels to share the same decrement from the baseline (i.e. no problem).
Table 4 presents Irish data, with Australian and the UK data provided in the supplementary materials (Appendix 2, Tables 2a-c). The comparison between context and no-context scenarios shows mixed results across different dimensions and study arms. In study arm 1 (3-month life expectancy with limited support), while some dimensions like mobility and self-care showed larger decrements in the context scenario (for example, MO5: -0.555 vs -0.374; SC4: -0.287 vs -0.215), this pattern was not consistent across all dimensions. For instance, in usual activities, the context decrements were actually smaller or similar to no-context decrements (UA4: -0.106 vs -0.135; UA5: -0.235 vs -0.261), and in anxiety/depression, the extreme level showed similar magnitude but slightly smaller decrement in context (AD5: -0.305 vs -0.326). Across study arms 2–4, the patterns remained variable, with differences between context and no-context scenarios showing no consistent direction or magnitude. For example, in study arm 3, some decrements were larger in the context scenario (SC5: -0.378 vs -0.256), while others showed the opposite pattern (MO2: -0.076 vs -0.147). The variability in the data suggests that the influence of palliative care context on health state valuations appears to be less systematic than might have been hypothesized.
Table 4 Anchored and adjusted EQ-5D-5L decrements in the Irish sampleThe Australian data (Appendix 2, Table 3a) shows similar variability but with generally larger magnitude coefficients. For instance, in study arm 1, mobility level 5 shows stronger context effects (MO5: -0.606 vs -0.467) compared to the Irish data. The UK data (Appendix 2, Table 3c) also demonstrates mixed patterns. For example, in study arm 1, mobility level 5 shows similar context effects to Australia (MO5: -0.607 vs -0.532), but other dimensions show more modest differences between context and no-context scenarios.
Across all three countries, the impact of palliative care context on health state valuations showed variable patterns across different scenarios, with no clear evidence that the worst-case scenario (study arm 1) consistently produced larger decrements compared to milder scenarios. The influence of context appeared to be more complex and less dependent on scenario severity.
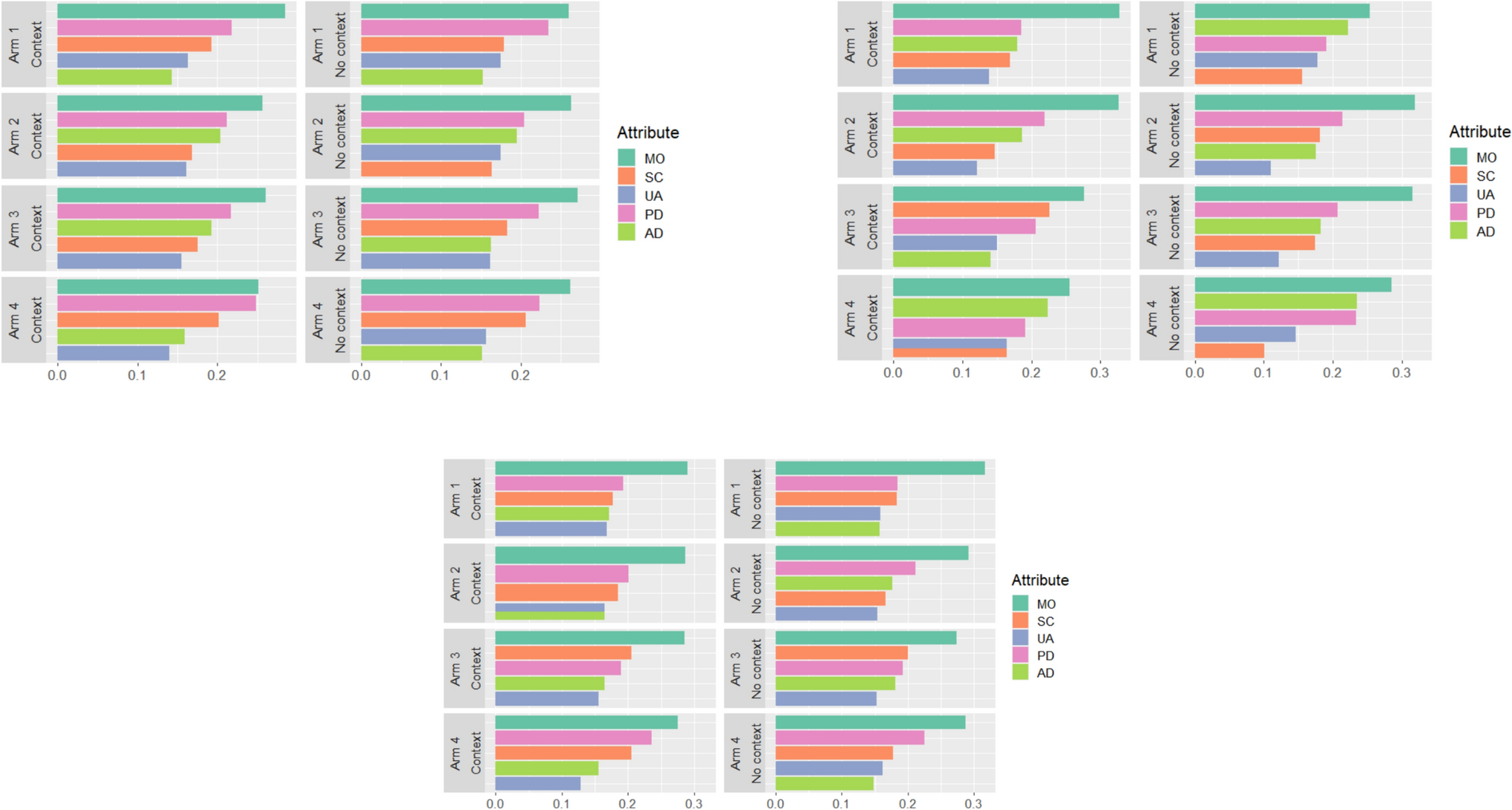
Figure 1 illustrates the relative importance scores across Australia, Ireland, and the UK for the four study arms. Mobility consistently emerged as the most important attribute in all three countries, regardless of variations in the contexts. In Irish Arm 1, one interesting observation is that the importance of mobility was comparatively lower under the no context scenario, compared to the worst-case scenario (i.e. a 3-month prognosis and limited support). In addition, preference heterogeneity was observed, as indicated by the variations in RAI scores under the no context scenarios among different study arms. However, when comparing RAI scores between palliative care context and no context scenarios, only minor differences were observed across four study arms and three countries.
Fig. 1
Relative attribute importance in three countries. a Relative attribute importance in the Australian sample. b Relative attribute importance in the Irish sample.: Arm 1, Context: a 3-month life expectancy with limited support; Arm 2, Context: a 3-month life expectancy with adequate support; Arm 3, Context: a 2-year life expectancy with limited support; Arm 4, Context: a 2-year life expectancy with adequate support
The impact of context on preferences for the “death” health stateOverall, the number of health states worse than dead was largest in the Australian sample, while the Irish sample had the lowest number of such states (Fig. 2). In addition, the impact of palliative care contexts was evident in the percentages of health states worse than dead, with the most significant effect in the worst-case scenario (arm 1: the palliative care context with a 3-month life expectancy with limited support). Specifically, under the no context scenario, there were 15.5%, 5,3% and 12.2% health states considered to be worse than dead in Australia, Ireland, and the UK respectively. These percentages increased when respondents were presented with the palliative care scenario (arm 1: a 3-month life expectancy with limited support), with 32.5%, 14.7% and 24.6% in Australia, Ireland, and the UK respectively.
Fig. 2
Influence of palliative care needs context on EQ-5D-5L health states considered worse than death by country
Comments (0)