Our data demonstrate correlations with enlarging MM classification and stoma-specific QoL. Specifically, image series rated as MM II were associated with a statistically significant difference in hernia-specific quality of life and stoma-specific quality of life vs non-recurrent (MM0) series. Reoperations for parastomal hernia recurrences were found to be related to stoma-specific quality of life and pain among patients who completed 1-year and/or 2-year follow-up after open retromuscular PSH repair. Together, these results align with primary PSH literature regarding size/classification, symptoms, and decisions around (re)operative intervention. While other studies almost exclusively consider primary PSH, this data provides key insights into the interpretation of radiographic studies, reoperative decision-making, and patient experiences regarding recurrent PSH following open RM repair.
MM classification and quality of life
The association between MM classification and a readily available QoL instrument is an important finding for multiple reasons. CT scans are frequently utilized in rPSH surveillance. Routine radiographic follow-up is often standard of care in clinical practice and research protocols; thus, clinical correlations with radiographic findings are essential to justify utilization of the technology and appropriately interpret findings [1, 6]. However, beyond characterization of a patient’s outcome as ‘herniation/recurrence’ or ‘no herniation/non-recurrent’ when summarizing post-operative PROs across groups, scant literature correlates symptom severity across a continuum of PSH sizes/radiographic classifications. Though the original MM system was designed to correlate imaging and exam findings with patient-reported symptoms, the determination of symptomatic vs asymptomatic was binary [7]. While patients with a PSH classified as MM II might have experienced greater symptom severity vs MM Ib, the system was not designed to account for such differences. No studies to-date have evaluated differences in symptom severity across each MM classification; recently, the largest systematic review of clinic-radiological accuracy of PSH was unable to identify literature associating radiographic recurrence classification with symptom severity [13]. While one study has validated the preoperative European Hernia Society Classification System of parastomal hernias (EHSC) for operative planning and captured post-operative QoLs, they did not report preoperative PROs, preventing stratification of symptom profiles across EHSC types [14].
Thus, the observation that MM correlates with the widely available CIS instrument is an important step in supporting the clinical relevance of the MM system. Our findings suggest utility for CIS as a potential post-operative surveillance screening tool for patients who could benefit from imaging to assess recurrence, regardless of stoma type. Further the observation of greater life impact for patients with MM II and MM III as determined by CIS, can inform surgeons’ interpretation of radiographs for patients with rPSH.
However, the observation of a higher median CIS score in the MM II vs MM III group, while not statistically significant, merits attention. Limitations in the utilization of a non-validated questionnaire or inadequate sample size could explain this; but the finding could also be inherent to the MM classification’s disregard of defect size and the static nature of CT scans. Patients with scans demonstrating MM II (herniation of non-bowel contents into the sac, namely, omentum), may actually have a defect aperture which accommodates bowel herniation while standing, prone, or with Valsalva (though not seen on imaging). As such, some literature has advocated for Valsalva or prone positioning to be part of all PSH radiographic protocols [15]; notably, though, the MM classification was validated only in supine patients without Valsalva [7]. For such patients, the risk of intermittent bowel obstruction may be the same or higher than MM III. Similarly, the presumably smaller defect of MM II PSH (vs MM III) may incur greater congestion at the defect neck as additional omentum herniates through, leading to partial obstruction of the stoma or omental infarction, both of which could induce discomfort or stoma dysfunction.
Quality of life and reoperation
Patient-reported pain and stoma burden on life were significantly elevated in patients receiving reoperation after RM PSH repair vs those without reoperation. Quality of life is a central consideration when offering patients parastomal hernia repair, and no guidelines currently provide recommendations for watchful waiting vs surgical management (regarding primary or recurrent PSH) [4]. However, the threshold to electively operate on rPSH is anecdotally higher than primary hernias. Recurrent PSH repair is associated with a higher rate of wound morbidity and recurrence [16, 17], which has been shown to increase with each subsequent repair [18]. While our study did not capture PROs following reoperation (as patients were said to have met the primary endpoint of the index trial upon receiving a reoperation for recurrence), this would be an important step for future efforts.
Our data does, however, make direct comparisons regarding patient-reported quality of life between patients with recurrence at the time when reoperative decision-making occurred, identifying factors which likely prompted consideration of reoperation. When considering the magnitude of difference between reoperative and non-reoperative groups, the median non-reoperative PROMIS3a T score of 30.70 is the lowest possible on the scale, whereas the median reoperative score of 60.50 is the 4th highest (for PROMIS3a v1.0). Pain, as it relates to PSH, has been discussed previously and multiple studies have identified a correlation between patient-reported generalized pain and onset of PSH [19,20,21]. By implementing multiple QoL surveys featuring pain, Krogsgaard et al. [22], appeared to isolate stoma site pain as the primary driver of this association. Only one study has previously demonstrated a link between recurrence and pain, wherein 7 of 77 patients recurred after mesh-based PSH repair and all 3 patients with new onset chronic pain were in the recurrence group [23]. In our study, PROMIS 3a score did not differ across MM groups, nor in our analysis of the MM Ib-exclusive recurrence definition. Instead, our results suggest a role for PROMIS3a in post-operative surveillance of PSH— not to detect recurrence, but to identify patients who may require reoperation.
As with MM classification group, our results associated CIS with reoperation. Notably, however, the median score in both patient groups (non-reoperative and reoperative) was greater than 10 (11 vs 22, respectively) indicating a “major” life impact of the stoma. Given our other results demonstrating the utility of CIS in capturing negative outcomes of PSH, it is not surprising that the CIS score was higher in patients who ultimately required reoperation. However, that the median score for all patients was above the threshold for “major life impact” was unexpected. Timing of data collection may have contributed to this finding. The CIS was initially validated with survey results from patients at a mean 4.6 years following stoma creation [10]. Patient ‘response shifts’ over time have been demonstrated to influence QoL scores, with trends toward improvement over time [24, 25]. In contrast to this, one study failed to identify a difference in QoL scores at < 12 months vs > 12 months after stomal surgery; however, their mean follow-up for the > 12 month group was not reported [26]. We did not observe a meaningful difference between patients in the 1 year vs 2 year groups regarding any of the QoL measures, and any further analysis of a time-dependent effect is outside the scope of this investigation. Alternatively, the increased discomfort/burden could be attributed to the RM repair with PCS. While the technique [6] and early surgical outcomes [27] have been previously reported in literature, our study represents the only study to-date reporting patient QoL following RM SB and KH repairs and this finding may be novel. As such, further investigation is required to characterize patient-reported outcomes in addition to surgical outcomes, which have been given far more attention [28,29,30,31,32].
Recurrence and reoperation — can imaging guide management?
For the purpose of defining PSH as a research outcome— whether primary PSH after the utilization of prophylactic mesh or rPSH following repair— current literature is variable. In a 2020 systematic review [13], only 62% of studies included a definition, and among these 19 different definitions were identified. Eight of these were based on radiographic findings alone. Classification was only considered in 45% of studies, most of which utilized MM, then the EHSC, and a minority featured both. The MM classification system both defines and classifies PSH using imaging modalities that are now widely available in clinical practice, making it a useful instrument in research.
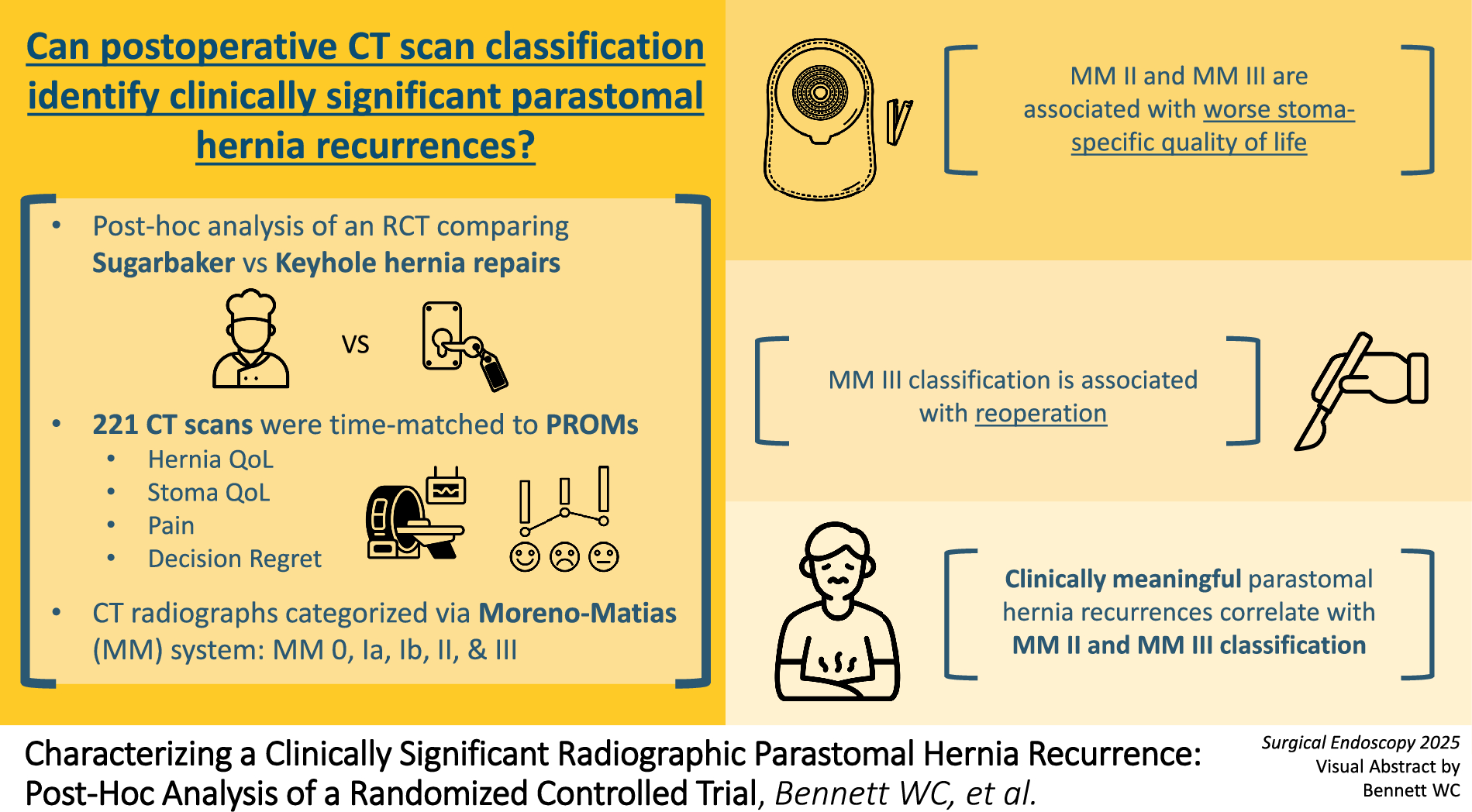
However, the current MM definition of a “true hernia,” and thus recurrent hernias following repair, may diagnose PSH recurrence in patients without clinically significant symptoms. The rate of PSH recurrence is known to be high, but a minority of patients undergo reoperation, suggesting excessive sensitivity for recurrence by contemporary diagnostic schema and inadequate specificity for clinically meaningful disease. As mentioned, the MM Ib-inclusive definition of a clinically significant PSH in the original study by Moreno-Matias only regarded a binary determination of ‘symptomatic’ and did not consider symptom severity. However, our data demonstrate worsening stoma-specific quality of life for patients with MM II, rather than MM Ib, and support a stricter definition of recurrence starting at MM II. While no statistically significant differences between MM Ib or other groups were detected (likely due to sample size constraints), MM II was demonstrated to be different from MM 0 regarding abdominal wall-specific QoL and stoma-specific QoL. Further, the subsequent Cohen’s effect size difference analysis suggested less difference between MM Ib and the classically non-recurrent groups (MM 0 and MM Ia) regarding stoma-specific quality of life, pain, and decision regret. Given the limited sample sizes of the non-MM 0 groups, the analysis was underpowered, and the results are not statistically. However, they are highly suggestive of a symptomatic delineation occurring between MM Ib and MM II.
Regarding reoperation— arguably the most salient indicator of a clinically significant recurrence— only recurrences classified as MM II and MM III from the primary dataset were observed to have undergone reoperation for true recurrence. The MM 0-classified reoperation included above was for a prolapsing stoma, which does not meet the majority of accepted definitions of PSH; however, we did not prespecify this exclusion and chose to include it in the final analysis. Notably, there was one patient from the MM 1b cohort who underwent reoperation but was excluded from the initial analysis due to an absence of time-matched PROs. When the reoperative patients without PROs were included, the reoperation rate for MM Ib was 4.17%; far lower than the 22.58% reoperation rate observed for MM III-classified recurrences.
Altogether, our data suggest the clinical significance of a recurrent PSH corresponds with an MM II classification or greater, defined as the point at which cross-sectional imaging detects extraperitoneal displacement of intraperitoneal contents. Patient-reported outcome measures demonstrate a decline in QoL once characterized as MM II, and reoperation rates are significantly elevated for image series with MM III classifications. Thus, an MM II recurrence definition is effective for characterizing and detecting clinically significant PSHs which may benefit from stoma nursing or counseling on possible reoperation.
The utility of MM classification in guiding reoperative decision-making is a novel finding which has not been previously demonstrated [4]. Only a single retrospective study [33], which excluded rPSH, has investigated radiographic PSH classification systems’ with eventual need for operative repair of PSH. They found an association with the EHSC type, but not MM type among 62 patients with PSH, 27% of which underwent reoperation. They observed EHS Type III (no concomitant midline and defect size > 5 cm) PSHs were less likely to undergo reoperation than Type I (no concomitant midline and defect size ≤ 5 cm) PSHs. This finding is loosely discordant with our findings. While MM does not consider defect size, presuming MM III defects are larger than MM II defects, we observed reoperation rate to increase with increasing MM class. This discrepancy could represent differences in group practice patterns as both were single-center studies, decision-making regarding primary PSH vs rPSH, or decision-making following open RM repairs in particular. Further studies stratifying reoperative decision making and outcomes across classifications are certainly required to better understand the predictive utility of these systems.

Comments (0)