
Remember me
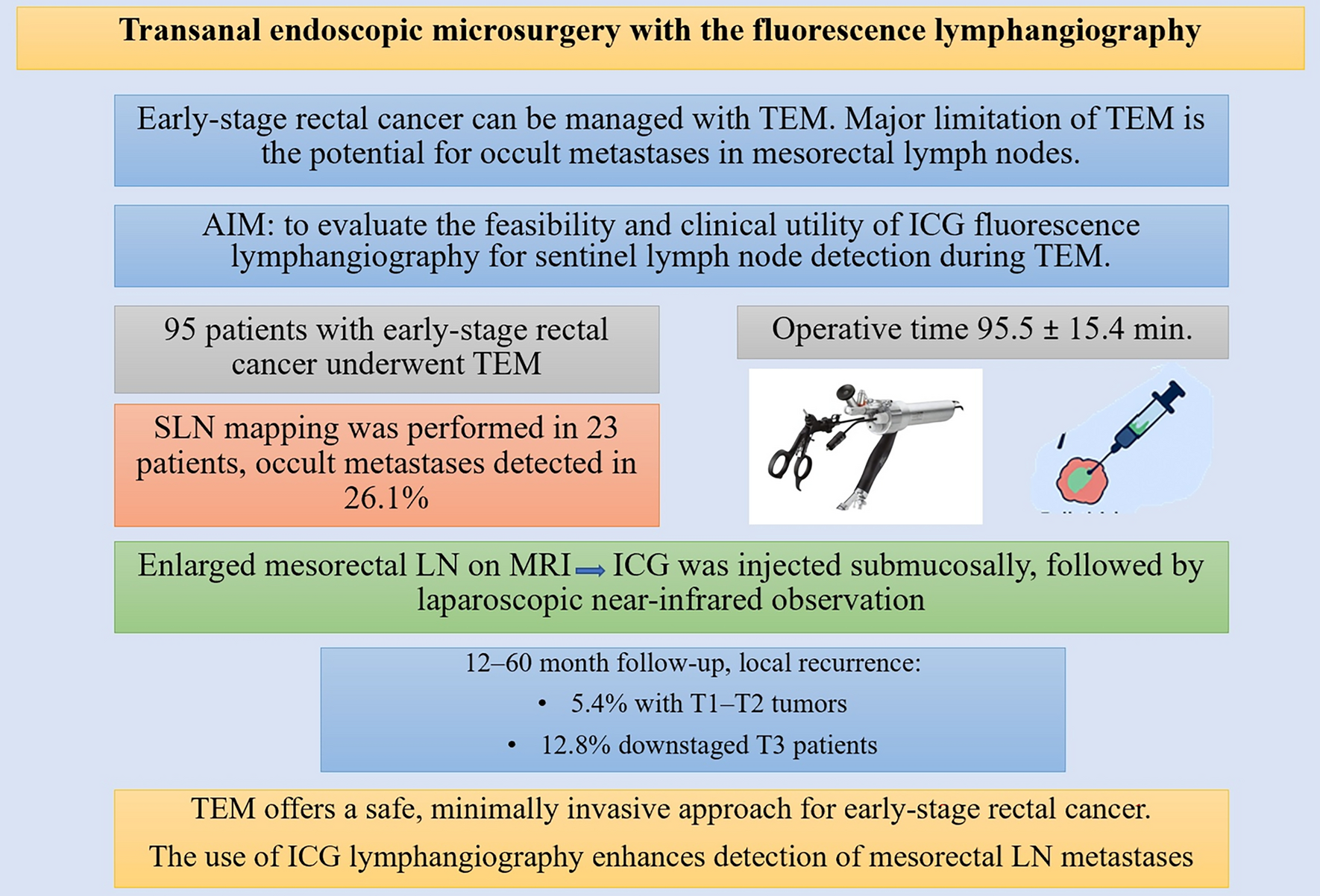
Early-stage rectal cancer can be managed with transanal endoscopic microsurgery (TEM) as a minimally invasive alternative to radical surgery. However, a major limitation of TEM is the potential for occult metastases in mesorectal lymph nodes.
ObjectiveTo evaluate the feasibility and clinical utility of indocyanine green (ICG) fluorescence lymphangiography for sentinel lymph node detection during TEM.
MethodsA total of 95 patients with early-stage rectal cancer underwent TEM using a rigid rectoscope platform (Karl Storz TEO, Germany). Full-thickness local excision with 1–2 cm margins and primary defect closure was performed. In patients with enlarged mesorectal nodes on preoperative MRI, 5 mg of ICG was injected submucosally around the tumor, followed by laparoscopic near-infrared observation and sentinel node excision for pathological analysis.
ResultsFrom 2009 to 2024, 95 patients (52 men, 43 women; mean age 67.4 ± 7.2 years) underwent TEM. The mean operative time was 95.5 ± 15.4 min. Postoperative complications occurred in 7 patients (7.4%), primarily bleeding and pulmonary events; no anastomotic leaks or perioperative mortality were observed. Sentinel lymph node mapping was performed in 23 patients, with occult metastases detected in 6 cases (26.1%). These patients were advised radical resection with total mesorectal excision (TME); 4 underwent TME, and 2 opted for chemotherapy. During a 12–60 month follow-up, local recurrence occurred in 3 of 56 patients with T1–T2 tumors (5.4%) and in 5 of 39 downstaged T3 patients (12.8%).
ConclusionsTEM offers a safe, minimally invasive approach for early-stage rectal cancer. The adjunct use of ICG lymphangiography enhances detection of mesorectal lymph node metastases and helps identify patients who may require additional radical surgery with TME.
Graphical abstract
Comments (0)