Comparison of Applicator-Based Point A and Anatomical Point A in Terms of Position and Dosimetry in Intracavitary Brachytherapy (ICBT) for Carcinoma Cervix Patients
Purpose
To evaluate the spatial and dosimetric differences between traditional applicator-based point A and anatomically defined point A in cervical cancer brachytherapy.
Materials and Methods
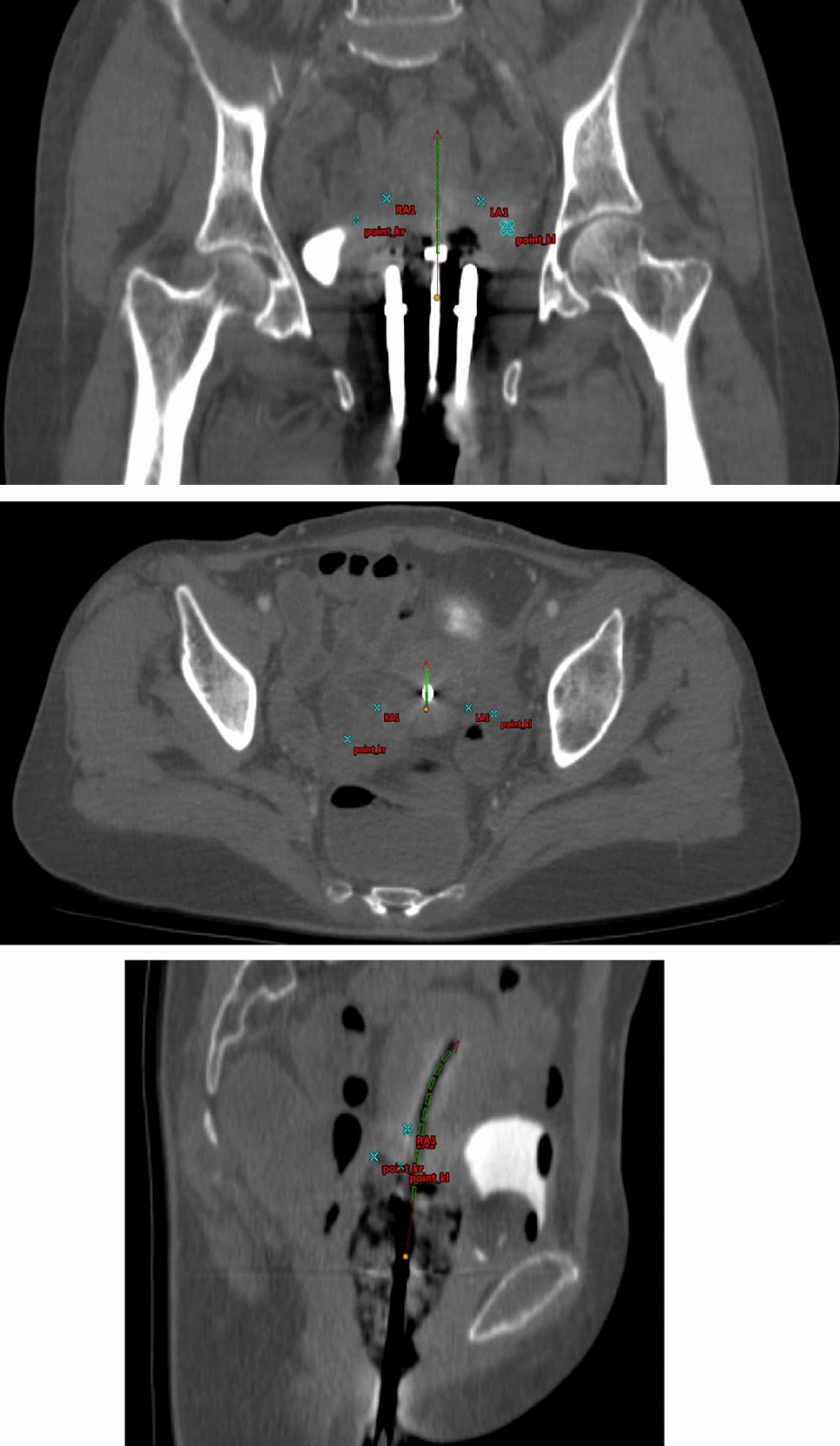
Thirty cervical cancer patients post-external beam radiotherapy underwent ICBT HDR brachytherapy. CT simulation was performed in arterial (15–30 s), venous (2 min), and delayed (8 min) phases. Anatomical point A was identified at the intersection of the uterine artery (arterial phase) and ureter (delayed phase). 7 Gy was prescribed to applicator-based point A, and the spatial relationship between both points was analysed.
Results
Anatomical point A was superior in 40% and inferior in 60% of cases. The mean distances from applicator-based point A were: right side—1.1 cm superior, 1.38 cm inferior, 1.71 cm lateral, 1.9 cm anterior, 0.91 cm posterior; left side—0.81 cm superior, 1.33 cm inferior, 1.76 cm lateral, 1.07 cm anterior, 0.34 cm posterior. Applicator-based point A was inside the uterus in 50% of cases, at the uterine wall in 27%, and outside in 23%. Anatomical point A was always extrauterine. When prescribing to applicator-based point A, anatomical point A received 48% less dose, while applicator-based point A received 128% more when prescribed to anatomical point A (p < 0.05).
Conclusions
Point A needs to be redefined, and further studies are required to establish consensus on the prescription point in ICBT HDR, emphasising the preference and feasibility of volume-based planning.

Comments (0)