
Remember me
A total of 2903 cases of lymphoma were diagnosed during this period. One thousand and ninety-one cases were Hodgkin’s lymphoma (37.5%), and 1812 cases were diagnosed as non-Hodgkin’s lymphoma (62.5%). Six cases of ovarian non-Hodgkin’s lymphoma (0.2% of all lymphoma cases) were detected, out of which, in three cases, ovaries were involved as part of systemic involvement. In the other three cases, ovary was the primary site of involvement. All the three cases of our present study were B-cell non-Hodgkin’s lymphomas.
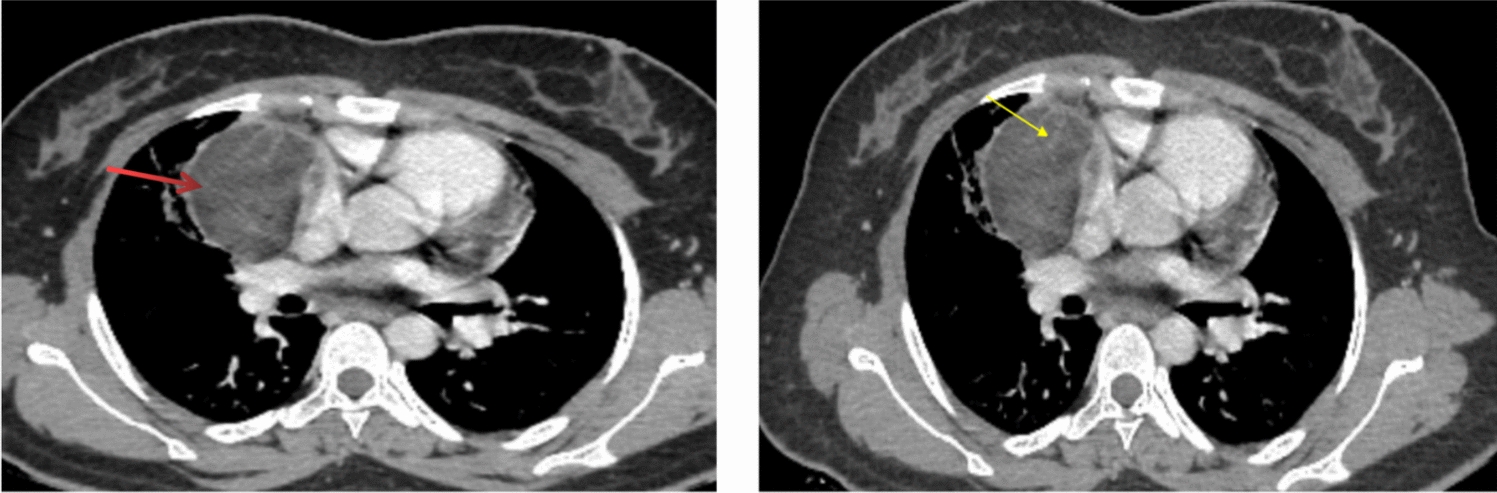
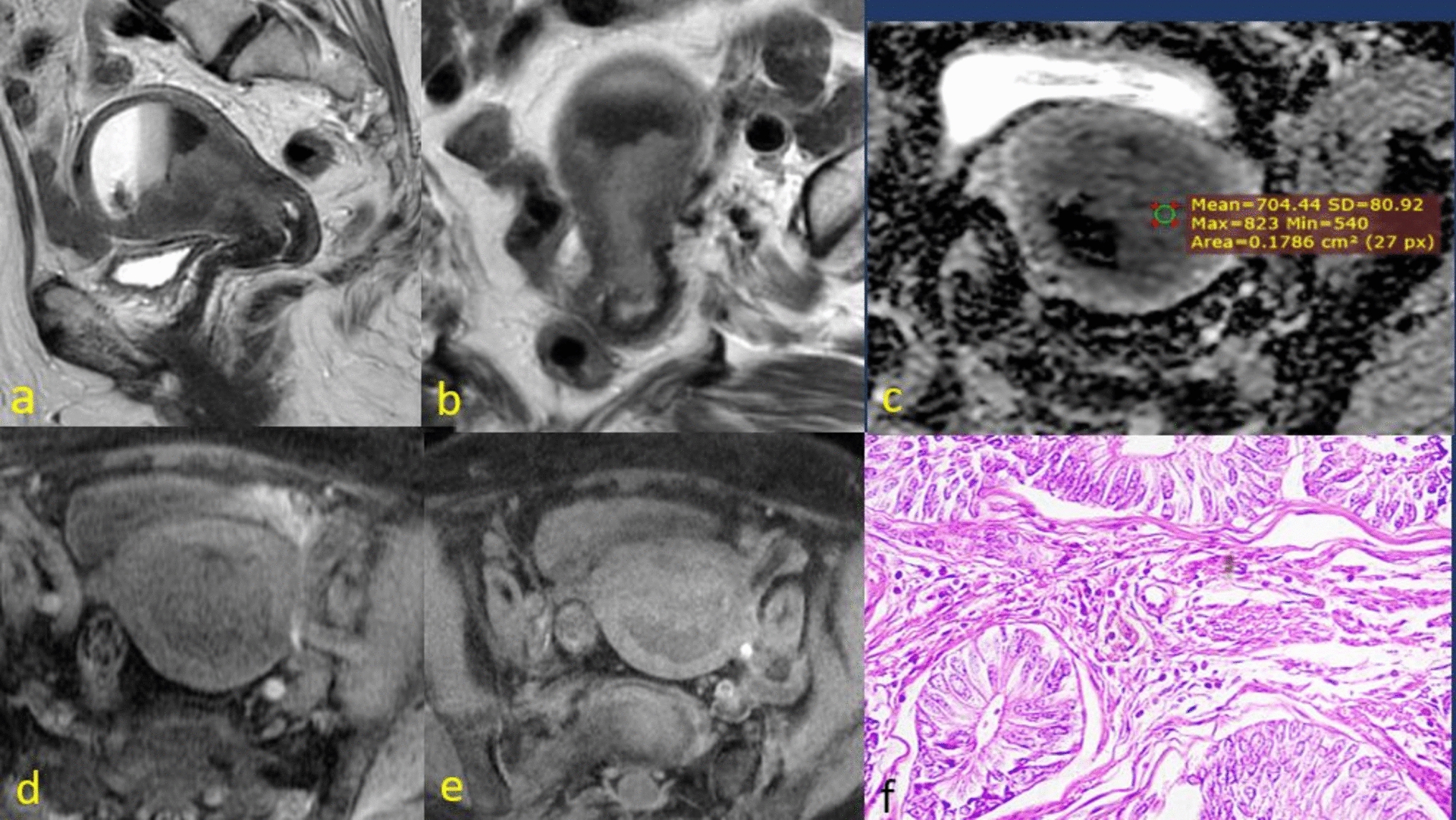
Our first case was a 45-year-old multiparous woman presented with lower abdominal pain for 4 months and lower back pain for the past week. She had no significant medical or family history and was not taking any medications. Physical examination revealed a tender mass in both iliac regions extending to the umbilical area. Her CA-125 level was elevated to 257 U/mL, while other tumor markers were normal (CEA 1.73 ng/ml and CA-19.9 8.98 U/ml). CT scan of abdomen and pelvis showed predominantly solid, heterogeneously enhancing bilateral adnexal masses measuring 13 × 7 cm on the right and 9.2 × 7.3 cm on the left, with loss of fat planes between the masses and the sigmoid colon as well as the bowel loops (Fig. 1A, B). An additional well-defined lesion was noted along the left lateral wall of the uterus measuring 2.2 × 2.1 cm. Enlarged retroperitoneal lymph nodes were also noted, the largest being 1.2 × 1.1 cm in the left para-aortic region. A biopsy from the pelvic mass was performed, which came about as leiomyoma. The patient concurrently developed ascites, and fluid analysis revealed the presence of malignant cells. However, due to the limited volume of fluid, a cell block could not be prepared. Immunohistochemistry was recommended for further tumor characterization.
Fig. 1
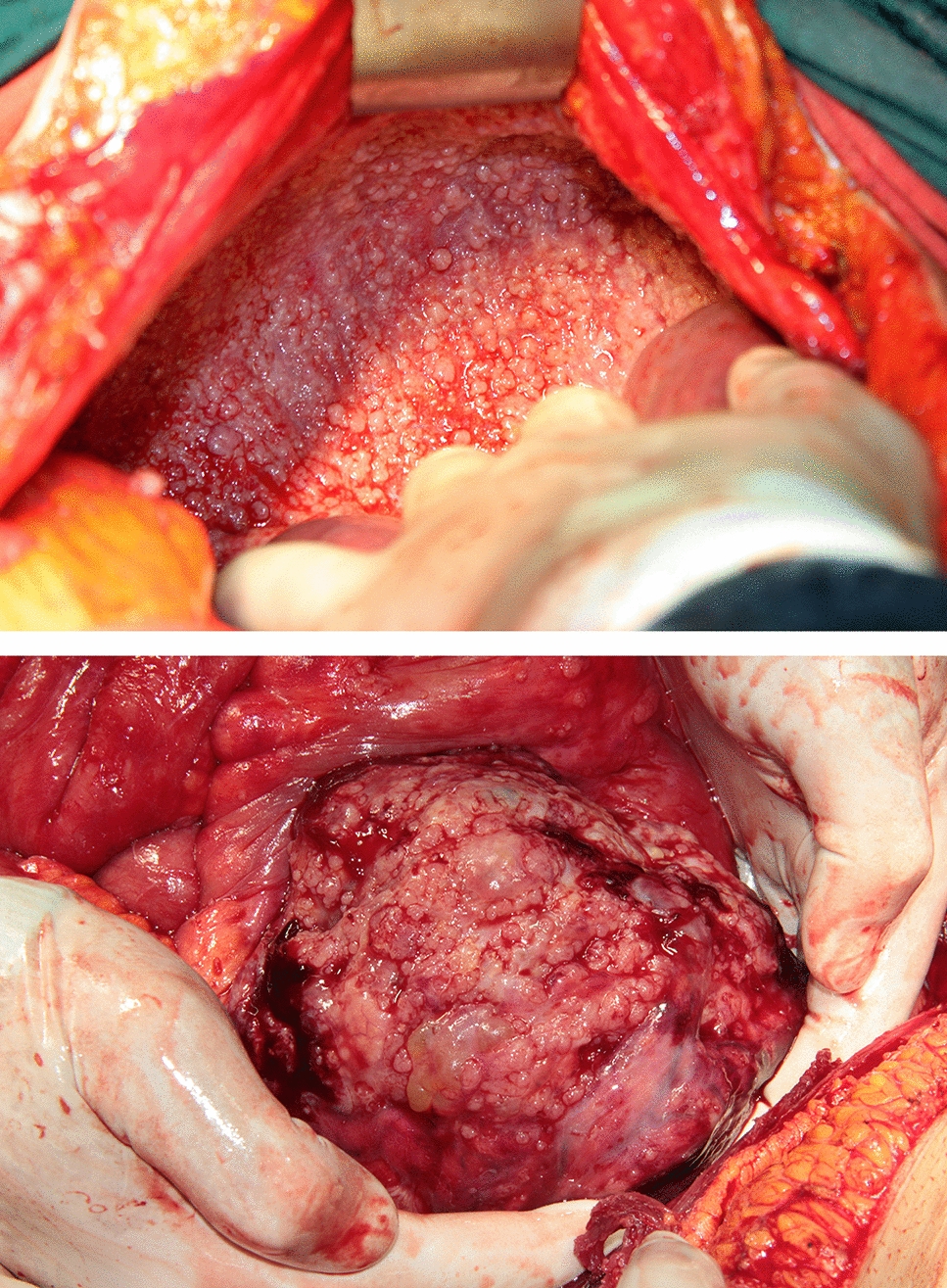
(Case 1): A, B Coronal and axial CT images show solid heterogeneously enhancing bilateral adnexal masses. Free fluid is also seen in pelvis. C, D Frozen section images show sheets of large atypical cells having pleomorphic nuclei lying over a sclerotic stroma. Numerous mitotic figures are seen (arrows). Many tumor giant cells and bizarre nuclei are also noted (arrow heads) [H&E, 40X]. E,F Gross picture of the bilateral adnexal masses showing solid gray–white tumors
Eventually, the patient was scheduled for a total abdominal hysterectomy with bilateral salpingo-oophorectomy with intra-operative frozen section for primary diagnosis of the adnexal masses. Bilateral adnexal masses were sent for frozen sectioning. Four–5 micron thick sections were cut using the cryostat machine, and H&E staining was performed. Sections from both the masses showed similar morphology. Both the ovaries were completely replaced by tumor cells which were markedly pleomorphic, having irregular, hyperchromatic nuclei, and prominent nucleoli. Many tumor giant cells and bizarre cells were noted. Stroma was densely sclerotic. Brisk mitosis was noted. With this morphology, a diagnosis of poorly differentiated malignancy, possibly high-grade malignant mesenchymal tumor was suggested (Fig. 1C, D).
Based on the frozen findings, an extensive surgery was performed, and specimen of total hysterectomy with bilateral salpingo-oophorectomy with infracolic omentectomy, bladder surface peritonectomy, and pelvic lymph node dissection with complete cytoreduction and was sent for histopathological evaluation. The uterus measured 7 × 6x4cm, right ovary measured 14 × 12x10cm, left ovary measured 15 × 13x8cm, and right and left fallopian tubes measured 5 × 1 cm and 5.5 × 1 cm, respectively. Omentum measured 20 × 10x0.3 cm. Cut sections of the ovaries showed solid, gray–white masses without capsular breech or serosal deposits (Fig. 1 E, F).
Microscopic examination of the tumor sections revealed ovarian tissue infiltrated by large atypical cells with coarse nuclear chromatin and scant cytoplasm. Many bizarre tumor cell nuclei and multinucleated tumor giant cells were noted. Areas of necrosis with perivascular accentuation of tumor cells were seen. Numerous mitotic figures were present including many atypical forms. Perineural invasion was also identified (Fig. 2 A–F). While the uterus, cervix, and bilateral parietal parametria were free of tumor, both cornua and bilateral fallopian tube were involved, and multiple deposits were also found in the omentum and bladder peritoneum. Based on the morphology, the primary differential diagnoses considered were high-grade malignant mesenchymal tumor, high-grade epithelial tumor, and embryonal carcinoma.
Fig. 2
(Histomorphology, Case 1): A Microsection shows sheets of large round cells having prominent nucleoli, [H&E, 40X]. B Another area from the same tumor shows numerous multinucleated tumor giant cells and bizarre tumor cells over a sclerotic stroma, [H&E, 40X]. C Areas of necrosis with perinuclear accentuation of tumor cells are noted, [H&E, 20X]. D Numerous mitotic figures are seen (arrows), [H&E, 40X]. E Perineural invasion of the tumor cells is noted, [H&E, 20X]. F Scanner view shows the involvement of fallopian tube by the tumor cells, [H&E, 4X]
The primary panel of immunohistochemical markers showed that tumor cells were negative for Pan-CK, Pax8, SMA, H-caldesmon, SALL-4, and CD30. With this panel of markers, the possibility of ovarian carcinoma, leiomyosarcoma, and germ cell tumors were ruled out. S 100, HMB45, and Melan A were also negative, thus ruling out malignant melanoma. INI1 was retained by tumor cells. Inhibin, SF-1, and calretinin were also negative, which ruled out possibility of sex cord stromal tumors. But the tumor cells were diffusely positive for LCA. Further panel of markers revealed CD20, BCL6, and MUM1 positivity in these cells. CD3 highlighted the background reactive T cells, while CD10 and c-myc were negative. Ki-67 proliferative index was 85% (Fig. 3 A–D). Based on these findings, a final diagnosis of diffuse large B-cell lymphoma, activated B-cell type was rendered. The tumor was clinically classified as Stage IV. Within a week of the report release, the patient underwent one cycle of prephase chemotherapy. However, her condition began to deteriorate shortly afterward. A bone marrow aspirate planned for staging was postponed due to her rapid decline. Unfortunately, she passed away from disease progression within a month.
Fig. 3
(Immunohistochemistry, Case 1): A Tumor cells are diffusely positive for CD45, [H&E, 40X]. B CD20 is positive in the tumor cells, [H&E, 40X]. C MUM1 shows nuclear positivity, [H&E, 40X]. D High Ki-67 proliferative index in the tumor cells, [H&E, 40X]
Second case was a 17-year-old girl presented in respiratory distress with a large abdominal mass, ascites, and bilateral pedal edema. She had no notable medical or family history and was not on any medications. During the physical examination, a large, palpable mass was found in the lower abdomen, involving the anterior abdominal wall. Laboratory tests revealed low hemoglobin at 8.6 g/dL. Serum CA-125 level was raised to 121.3 U/ml. All other tumor markers were within normal limits, including serum THCG and serum AFP. Serum LDH was not done at baseline. A CT scan of the chest, abdomen, and pelvis showed a large hypodense pelvic mass measuring 11 × 8.6 × 11 cm, with a cystic component and, loss of fat planes with the rectum, recto-sigmoid junction, urinary bladder, and uterus, extending to the umbilical region while also involving the anterior abdominal wall and subcutaneous fat (Fig. 4A). The mass compressed the bilateral external iliac veins.
Fig. 4
(Case 2): A Axial CT image shows solid heterogeneously enhancing adnexal masses. B Microsection shows sheets of malignant small round cells, [H&E, 20X]. C On immunohistochemistry, tumor cells are diffusely positive for CD45. D CD20 is positive in the tumor cells, E CD10 is positive, F TDT is diffusely positive in all the tumor cell nuclei, G CD3 highlights the background T cells, and H Ki-67 proliferative index is > 90%
Initially suspected to be a primary ovarian malignancy, the patient underwent adnexal mass biopsy. Histological analysis revealed sheets of polygonal cells displaying round nuclei, dispersed chromatin, occasional with small nucleoli, and moderate amount of eosinophilic cytoplasm separated by fibrovascular septae. Interspersed small lymphocytes were also noted (Fig. 4 B).
Immunohistochemistry was put keeping in view of the morphology of malignant small round cell tumor. Initial panel of markers included Oct3/4, c-Kit, CD99, NKX2.2, and desmin. All these markers were negative, ruling out germ cell tumors, extra-skeletal Ewing sarcoma, and rhabdomyosarcoma.
On further testing, tumor cells showed diffuse positivity for LCA and negative for Pan-CK proving it to be a lymphoproliferative neoplasm. CD20, CD79a, TdT, and CD10 came out to be positive, with a very high MIB-1 labeling index (~ 90%). MUM1, BCL2, BCL6, and c-MYC were negative, leading to a diagnosis of precursor B-cell lymphoblastic lymphoma (Fig. 4 C–H). By that time, serum LDH was tested, which was raised (1362 U/l). Following this diagnosis, bone marrow examination was done which did not show involvement by atypical lymphoid cells. Unfortunately, the patient died due to the disease shortly thereafter before the chemotherapy could be started.
Our third case was a 14-year-old girl presented with abdominal swelling, fever, bilateral leg swelling, facial swelling, and shortness of breath for the past 20 days. Examination revealed large masses in both iliac fossae, measuring 10 cm and 7 cm. The initial tumor markers for germ cell tumors, beta-HCG, and AFP were within normal limits. Serum CA-125 was advised, which was found to be raised to 279 U/ml. Serum LDH value was also raised (1453 U/l). A CT scan of abdomen and pelvis showed bilateral solid adnexal masses, measuring 11.3 × 8.5 cm on the right and 12.1 × 9.5 cm on the left, displacing adjacent bowel loops but with no infiltration. There was also diffuse omental caking and nodularity. Due to widespread peritoneal disease with omental caking, nodularity, and bilateral adnexal masses suspicious for high-grade ovarian epithelial malignancy, an initial adnexal biopsy was performed.
Microscopy revealed fibrocollagenous tissue with diffuse infiltration by medium-sized tumor cells arranged in nests and separated by thin fibrous septa. The tumor cells had monomorphic nuclei, finely clumped chromatin, prominent nucleoli, and scant cytoplasm. Numerous macrophages were noted interspersed between the tumor cells. Immunohistochemical analysis showed positivity of the tumor cells for CD45, CD20, CD10, c-myc, and BCL6, while CD3, TDT, and CD34 were negative, leading to a diagnosis of Burkitt lymphoma. Ki-67 proliferative index was ~ 100%. Bone marrow biopsy showed no malignant cells, but cerebrospinal fluid examination was positive. The patient was classified as stage IV lymphoma and treated with the R-CYVE regimen. After 21 cycles of chemotherapy, she developed meningitis but was treated successfully. She has been followed for 24 months and is currently doing well.
The clinical and histochemical features of all three cases are summarized in Table 1.
Table 1 Clinical and histochemical features of three cases of primary ovarian lymphoma
Comments (0)