2.1 Study Design
This single-center, prospective, randomized, double-blind, placebo-controlled study was performed at Erasmus MC Sophia Children’s Hospital, Rotterdam, the Netherlands from January 2018 until May 2022. We investigated the hypotheses that WCI with ropivacaine leads to a morphine-sparing effect after abdominal surgery in infants aged < 1 year.
The Medical Ethics Committee of Erasmus MC approved this study on 21 June, 2017 (MEC-2017-074). This study was conducted in compliance with the current revision of the Declaration of Helsinki. Written informed consent was obtained from all parents or legal guardians of the children included in the study.
The study was registered in EudraCT (2015-002209-12) and the Dutch Trial Registry NTR6130 on 23 November, 2016 (International Clinical Trials Registry Platform NL-OMON20504). This manuscript adheres to the CONSORT guidelines.
Inclusion criteria were: children aged < 1 year, undergoing elective open abdominal surgery, post-conceptual age ≥ 35 weeks, and body weight ≥ 1500 g. Exclusion criteria were neurological disease, renal or hepatic dysfunction, receiving extra-corporeal membrane oxygenation therapy, long-term opioid or psychotropic drug (e.g., antiepileptic drugs, benzodiazepines, antidepressants) exposure pre- or postnatal, opioid exposure < 24 h before surgery, allergy to paracetamol, LA, or morphine, and contra-indications for RA (local or generalized infection).
2.2 Standard Anesthesia Protocol
Anesthesia was induced using propofol 1–4 mg/kg intravenously (IV) or by inhalation induction, using sevoflurane in a mixture of oxygen and air. Fentanyl 2 mcg/kg and rocuronium 0.6 mg/kg were administered IV before tracheal intubation. Anesthesia was maintained with sevoflurane at mean alveolar concentration (MAC) 0.7–1.0 in oxygen/air. Monitoring consisted of an electrocardiogram, non-invasive blood pressure, oxy-hemoglobin saturation, end-tidal CO2, and temperature. Additional doses of fentanyl 2 mcg/kg IV were administered, based on a heart rate or blood pressure increase. If possible, patients were extubated directly postoperatively. Children aged < 3 months (or < 60 weeks post-conceptual age in the case of prematurity) were admitted to the pediatric intensive care unit (PICU) postoperatively according to the local protocol.
2.3 Investigational Treatment
All children received a multi-hole wound catheter with holes over a trajectory of either 2.5 or 6.5 cm, depending on the length of the incision (On Q® Soaker Catheter; Halyard, Alpharetta, GA, USA). At the end of surgery, following closure of the muscle layers and fascia, the surgeon placed the wound catheter superficial to the muscle fascia under direct vision. The catheter was tunneled from a separate stab incision approximately 3 cm lateral to the wound. Thereafter, subcutaneous tissue and skin were sutured. The catheter was fixed to the skin using an adhesive plaster.
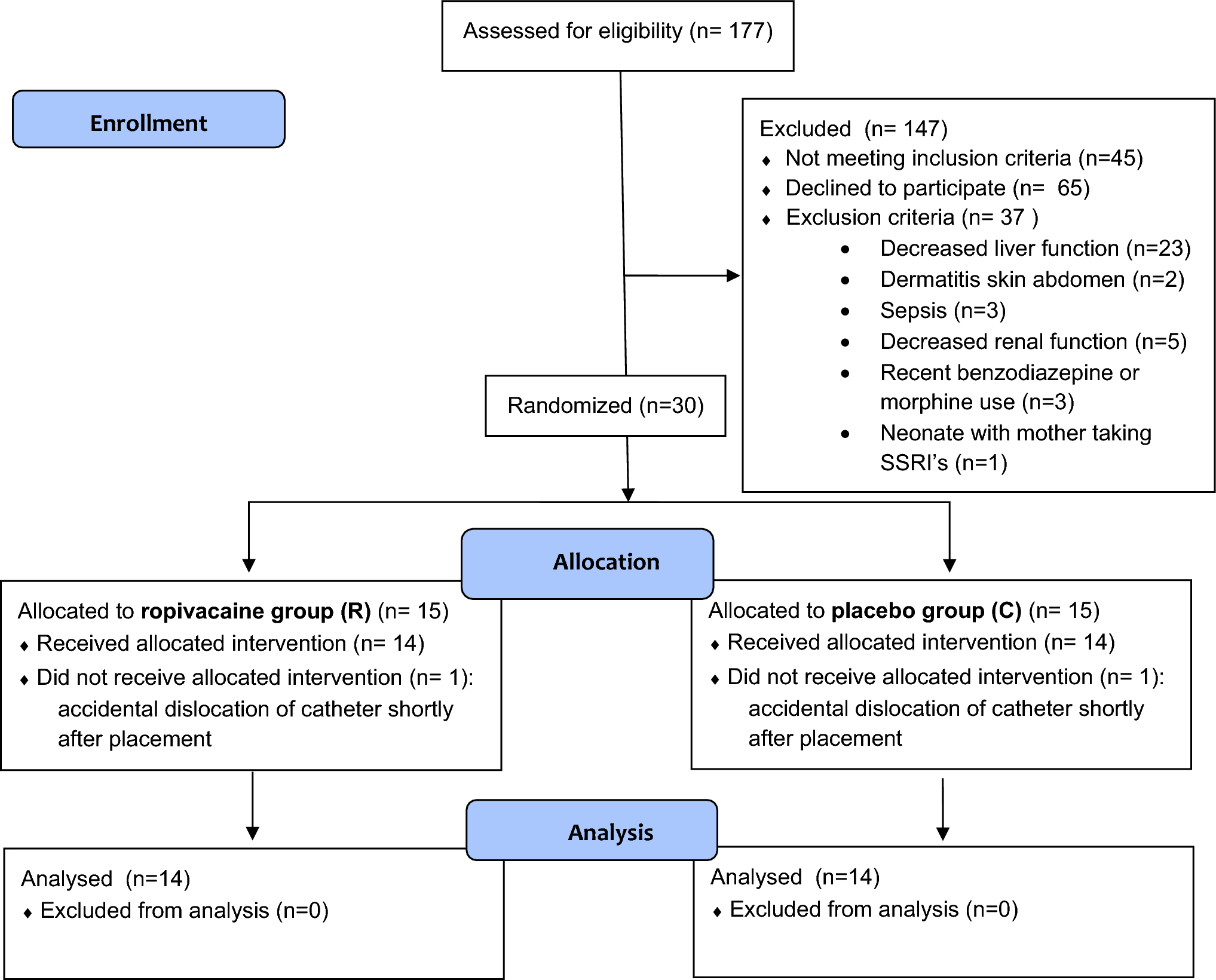
Included children were randomized for treatment with WCI with ropivacaine (R-group) or placebo (0.9% saline) [control or C-group], with 1:1 allocation. Hospital pharmacists performed randomization and prepared the blinded medication. A randomization schedule was made prior to the study, and codes were stored and kept solely by the pharmacist to ensure blinding until the end of the study. Surgical team, ward personnel, Acute Pain Service, and caregivers were all blinded to the treatment.
Before the end of anesthesia, the children received a bolus dose via the wound catheter of ropivacaine 2 mg/kg (= 1 mL/kg of ropivacaine 0.2%) (R-group) or the same amount of placebo (C-group). Thereafter, the wound catheter was connected to a syringe in a perfusor pump, administering a constant infusion of ropivacaine 0.1% at 0.2 mg/kg/h (R-group) or placebo (C-group).
At the end of the procedure, the C-group received a loading dose of morphine 100 mcg/kg IV to guarantee good analgesia at emergence of anesthesia in this group. The R-group received placebo IV.
2.4 Assessment and Treatment of Postoperative Pain
All patients received the first dose of paracetamol 20 mg/kg IV 30 minutes before the end of surgery. Intravenous paracetamol was continued postoperatively as a standard analgesic (60 mg/kg/day). In children aged 4 months and older, non-steroidal anti-inflammatory drugs, diclofenac or ibuprofen, were added to the standard analgesic regimen.
Postoperative pain was assessed every 2 h on the first day postoperatively, and after that on a regular basis, using the COMFORT Behavior Scale and Numeric Rating Scale (NRS) pain, as observed by the nurses [22]. Patients received rescue morphine doses, whenever the NRS was ≥ 4 and COMFORT ≥ 17, according to the local protocol, published by Ceelie et al. [23]. Doses of additional morphine 15 mcg/kg IV were administered every 10 min whenever needed, with a maximum of three times. Ten minutes after each extra dose of morphine, pain was reassessed. If there was no improvement, an additional dose of morphine 100 mcg/kg IV was administered and continuous morphine infusion was started. This could be increased, and other pain medication (esketamine, clonidine) or sedation could be added at the discretion of the attending physician. The infusion rate of WCI was kept constant until the removal of the wound catheter by the Acute Pain Service nurses at 72 h postoperatively.
2.5 Primary and Secondary Outcomes of the Study
The primary outcome of the study was the cumulative amount of morphine administered within the first 48 h postoperatively (mcg/kg) compared between both groups. Secondary outcomes were the number of patients needing extra morphine boluses within the first 48 h postoperatively, total amount of morphine administered postoperatively until removal of the wound catheter, area under the curve (AUC) over 24 h of COMFORT-B scores and NRS pain scores, percentage of high pain scores (NRS ≥ 4 and COMFORT ≥ 17), and the incidence of adverse events related to the wound catheter and the use of opioids and ropivacaine, including plasma concentrations of ropivacaine.
Adverse events related to the wound catheter and the administration of ropivacaine and opioids were recorded. Adverse events related to underlying disease and regular postoperative care were not recorded. Time until extubation, time until discharge from the PICU (if applicable), time to first feeding, and surgical stress score (SSS) were recorded [24]. An interim analysis of the primary outcome and safety (adverse events and plasma concentrations) was planned after the inclusion of 30 patients.
2.6 Plasma Concentrations of Ropivacaine
Samples for plasma concentrations of ropivacaine were collected until 72 h postoperatively, when venous blood sampling was needed for clinical purposes. Blood samples of 500 mcl were taken in CAT serum tubes and within 48 h these were centrifuged for 6 minutes at 20 °C with 3000 revolutions per minute. Plasma was stored in cryotubes at – 80 °C until shipment. The clinical pharmacology laboratory of the University Medical Centre Groningen, Groningen, the Netherlands analyzed total and unbound plasma concentrations of ropivacaine using liquid chromatography-mass spectrometry with a lower limit of quantification (LLQ) of 0.05 mg/L. If the total plasma concentration of ropivacaine was above the LLQ, free concentration of ropivacaine was analyzed further.
2.7 Sample Size Calculation
For the primary aim of the study, the calculation of the sample size was based on a previous study on the use of morphine postoperatively in children aged < 1 year after major surgery in our hospital [23]. We considered a 30% reduction in the cumulative morphine dose up to 48 h postoperatively in the R-group compared with controls to be clinically relevant. The number of patients required in each group was 26, as shown by a power analysis, in which the level of significance was 0.05 and the desired statistical power was 0.8. Considering a drop-out rate of 15%, the number of patients included in this trial was 60 (30 in each group). This sample size also provided sufficient power (> 80%) to detect a difference in the AUC of the COMFORT scores between groups with 0.8 standard deviations, using an independent samples t-test with a significance level of 0.05.
2.8 Statistical Analysis
Statistical analyses were performed using SPSS Statistics, version 28.0.1.0 (IBM Corporation, Armonk, NY, USA). The distribution of clinical characteristics was assessed using descriptive statistics. Primary outcome was compared between the randomization arms using the Mann–Whitney U test. Comparisons between randomization arms were performed using the Mann–Whitney U test for continuous variables and Fisher’s exact test for categorical variables. The AUC of the COMFORT and NRS scores during the first 24 h postoperatively were compared between randomization arms using the Mann–Whitney U test. A multivariable linear regression analysis was performed with the log-transformed values of cumulative morphine after 48 h as outcome and group allocation as predictors, and age, weight, gestational age at birth, and SSS as covariates.

Comments (0)