One of the most pressing issues in neonatal nephrology remains the accurate diagnosis and classification of acute kidney injury (AKI) in the early postnatal period. Neonatal AKI definitions continue to rely heavily on serum creatinine thresholds, despite the known limitations of this marker in the first weeks of life—when maternal creatinine is still present and tubular creatinine handling is immature. Dynamic assessments incorporating both direction and rate of creatinine change may offer a more physiologically sound approach, especially in very preterm neonates [20, 21].
Although not eligible for inclusion in the meta-analysis due to its younger age group (median age: 5 years) and absence of a term-born comparator, the FANCY study offers important corroborative evidence [22]. This prospective cohort study followed VLBW infants with and without a history of neonatal AKI. At follow-up, 65% of children with prior AKI showed signs of renal dysfunction—defined as reduced eGFR (based on cystatin C), elevated urine protein/creatinine ratio, or elevated blood pressure—compared to 14% in the no-AKI group. Notably, traditional creatinine-based eGFR calculations failed to detect any abnormalities, whereas cystatin C successfully identified reduced renal function in over one-quarter of the cohort. Although the FANCY study did not directly compare preterm infants to term controls, it indirectly reinforces the key message of the meta-analysis: subtle renal dysfunction is common and often under-recognized in preterm populations, especially in those with a neonatal history of AKI. Furthermore, the study raises the critical point that even stage 1 AKI may carry long-term consequences.
Children born preterm, particularly those with VLBW, are known to require more intensive healthcare during early childhood, with significantly higher rates of hospital readmissions and outpatient visits. While much of this increased healthcare utilization is clinically justified, some studies have highlighted substantial variability in follow-up strategies and hospitalization rates across centers and regions. This suggests that part of the care burden may result from institutional practice patterns rather than patient-specific needs. Although few studies have directly addressed the risk of over-hospitalization or over-surveillance in this population, the potential for inefficiencies or excessive medicalization—particularly among moderate or late preterm infants without major comorbidities—warrants further investigation. A more individualized, risk-adapted approach to long-term follow-up may help ensure that healthcare resources are used appropriately while avoiding unnecessary interventions.
In 2017, the Low Birth Weight and Nephron Number Working Group—a multidisciplinary international panel—published a seminal viewpoint that highlighted the long-term kidney implications of preterm birth and IUGR [24]. The report was among the first to emphasize the importance of structured nephrology follow-up in small vulnerable neonates, presenting nephron endowment not just as a developmental concept but as a measurable and potentially modifiable determinant of CKD and hypertension, calling for coordinated actions across obstetrics, neonatology, and nephrology. The group advocated for a developmental life-course approach, integrating prenatal, perinatal, and early postnatal risk factors to inform longitudinal kidney health strategies. It also suggested early and regular postnatal screening for infants born very preterm, growth-restricted, or with a history of neonatal AKI, including annual blood pressure checks and urinalysis starting from age 3, with earlier initiation in high-risk infants.
This early conceptual framework has since evolved into the more granular and operationalized protocol endorsed by the Neonatal Kidney Health (NKH) Consensus Workshop [25]. Specifically, the Consensus Workshop recommends the following:
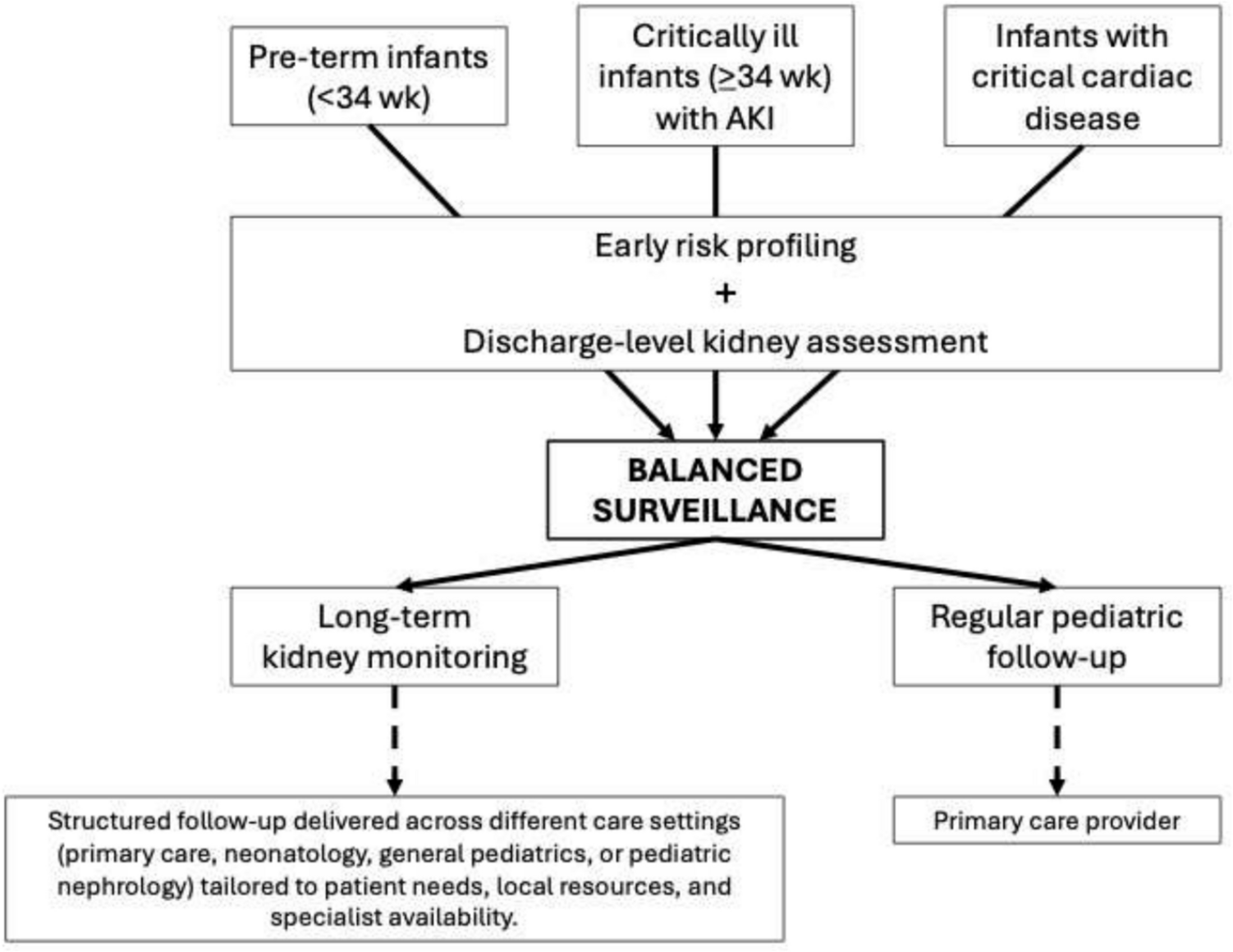
A baseline kidney health evaluation at the time of NICU discharge for all infants who experienced any stage of AKI, required dialysis, had severe neonatal comorbidities (e.g., ECMO, CDH, HIE), or received nephrotoxic medications. This evaluation should include properly measured blood pressure, serum creatinine, and family education.
A comprehensive outpatient nephrology follow-up within 6 months of discharge for high-risk infants (e.g., those with stage 2–3 AKI, dialysis, or complex multisystem disease). Follow-up should include serum creatinine and cystatin C, urine albumin-to-creatinine ratio, and eventually renal ultrasound.
A scheduled evaluation at 2 years of age for both high-risk and at-risk infants (e.g., those with stage 1 AKI or VLBW without AKI), including growth and blood pressure assessment, urinalysis, and kidney function tests.
Stratified follow-up beyond age 2, depending on interim findings and evolving clinical status.
Crucially, the consensus statement recognizes that serum creatinine alone is not sufficient to detect early renal impairment, especially in infants with reduced muscle mass or delayed growth trajectories. The use of cystatin C, alongside urinalysis and imaging, is promoted to enhance diagnostic sensitivity [26].
Equally important is the recommendation to not rely exclusively on the diagnosis of AKI as the trigger for long-term nephrology referral. A substantial proportion of infants who do not meet AKI criteria, often due to limitations in neonatal creatinine interpretation, may still present with reduced kidney function later in life. Thus, the evaluation of kidney health at discharge emerges as a pivotal moment in determining the need for follow-up. This includes reviewing serum creatinine trends, assessing blood pressure, evaluating urine output and proteinuria (if available), and performing imaging when clinically indicated.
The NKH consensus builds upon the conceptual framework proposed by the Low Birth Weight and Nephron Number Working Group, translating it into actionable, time-based surveillance recommendations [24, 25]. By combining early risk profiling with discharge-level renal assessment, it offers a pragmatic pathway to ensure that vulnerable infants are not lost to follow-up, even in the absence of overt neonatal AKI. At the same time, by focusing surveillance on those at highest risk, such an approach may also help to mitigate the risk of excessive medicalization and unnecessary interventions, striking a balance between vigilance and appropriateness. This strategy is aligned with the findings of the current meta-analysis by Dokousli et al., which shows that subtle yet significant alterations in kidney function, such as modest elevations in cystatin C, may be present in childhood despite a clinically uneventful neonatal course [11].


Comments (0)