
Remember me
CEUS is widely available as it only requires a US machine, and it is relatively inexpensive as only a few milliliters of contrast medium are used. Additionally, it is a safe method that can be used in nephropathic patients, regardless of creatinine levels, as the contrast medium is eliminated via the lungs [1,2,3]. CEUS also reduces the interobserver variability typical of US. Time-intensity curves allow for a quantitative assessment that, in the future, could help predict the biological behaviour of some renal lesions. Due to these positive characteristics, CEUS is mentioned in the European Association of Urology (EAU) guidelines with sensitivity, specificity, and negative predictive values approaching 100% [1, 4].
CEUS uses a contrast medium consisting of sulfur hexafluoride microbubbles stabilized by an external phospholipid shell. These microbubbles have a diameter smaller than 10 μm, so when injected intravenously, they pass through the pulmonary circulation without any problems. However, their size does not allow them to pass through the endothelium, so they are classified as blood-pool contrast agents. Under normal conditions, they do not escape the capillaries, meaning there is no extravascular phase, which causes a loss of information regarding capillary permeability and no urographic information, unlike computed tomography (CT) or magnetic resonance imaging (MRI) contrast agents. However, CEUS is extremely sensitive in studying microcirculation as the contrast medium remains confined to the blood vessels, combined with the maximum spatial resolution typical of US exams. In addition to qualitative evaluation of local perfusion, colorimetric maps can be created to assess microcirculation density, and time-intensity signal curves can be produced. The dynamics of renal contrast enhancement on CEUS are similar to what can be achieved with CT and MRI, except for the excretory urographic phase [5, 6]. The modality's limitations are the same as those of US: acoustic shadowing behind calcifications, acoustic shadowing behind intestinal gas, and beam attenuation in the case of deep lesions and patients with a high body mass index. There are also regulatory limitations as renal CEUS studies are currently off-label despite clinical evidence. Nonetheless, the European Federation of Societies for Ultrasound in Medicine and Biology (EFSUMB) has published specific guidelines for the use of CEUS in the uro-nephrological field. US contrast agents are physiologically safe (no need for preliminary laboratory tests, even in patients with liver disease or renal insufficiency). The literature reports a very low incidence of severe anaphylactoid reactions (0.001%). As mentioned, the components of US contrast agents (phospholipids) are eliminated by the liver in very small quantities (on average, 1.2–2.4 ml of contrast is injected), while sulfur hexafluoride is eliminated through respiration. There have been no fatal events in a series of 23,000 patients. These compounds are stable enough to last for the duration of a normal US exam (three to five minutes) [5].
The exam is usually performed with the patient in the supine or oblique position, elevating the side under examination. If there is meteorism of the colic flexures, a posterior approach with the probe placed at the level of the posterior axillary line or even more dorsally may be necessary. In these cases, the subcostal approach is not possible, and the study of the kidney must be done using the intercostal window, which does not allow visualization of the entire kidney in a single scan. In children and lean individuals, the prone position may be used due to the reduced thickness of the dorsal paravertebral muscles. If one or both kidneys are not identifiable in their normal location, the scan should be extended to the entire pelvis to search for ectopic and/or dysmorphic kidneys (presacral ectopia, horseshoe kidney, crossed ectopia). To determine the longitudinal diameter of the kidney, the best scanning plane should be found by moving the probe in real time so that both poles are well represented and the parenchymal thickness is uniform [7].
Principles of application of CEUS in the evaluation of renal lesionsThe characterization of renal lesions is a critical aspect of diagnostic imaging as it directly impacts clinical decision-making and patient management. Incidental renal lesions are frequently encountered in clinical practice, with US being the primary detection method, identifying 83% of cases compared to 15% for CT. However, B-mode US has significant limitations, particularly in distinguishing between solid and cystic lesions [8]. This distinction is essential as vascularized solid lesions are more likely to be malignant, necessitating further evaluation and intervention. Despite the widespread use of US and its availability, traditional US techniques, including color-Doppler, have been deemed insufficiently sensitive and specific by major guidelines. This has led to a growing interest in CEUS as a complementary and potentially superior imaging modality. Given the increasing clinical reliance on CEUS and evolving guideline recommendations, this review aims to provide a comprehensive analysis of its role in solid renal lesion assessment, highlighting its advantages, limitations, and future applications.
The American College of Radiology (ACR) as well as the EAU mentioned CEUS as a method that can be used with the same appropriateness as contrast-enhanced CT or MRI. CEUS helps overcome the main limitation of US, i.e., the lack of contrast medium, while also addressing the inherent limitations of the method, such as low accuracy and lack of specificity. CEUS also represents a valid alternative for better characterizing lesions that present pseudo-enhancement on CT, and consequently indeterminate lesions.
Ceus indications in renal imaging according to EFSUMB guidelinesCharacterization of Indeterminate Renal LesionsCEUS is not only useful for distinguishing between solid and cystic forms but also represents the first question a radiologist should ask when confronted with a newly discovered renal mass. For solid forms, CEUS allows the differentiation between pseudotumours (e.g., anatomical variants) and tumours (newly formed lesions) with higher sensitivity and specificity than CT (CEUS: SE 91%, SP 76%; CECT SE 85%, SP 64%) [3, 9] (Table 1).
Table 1 Comparison of renal pseudotumors and tumours, including their ultrasound (US) and contrast-enhanced ultrasound (CEUS) features. AVM arteriovenous malformation, RMC renal medullary carcinoma, SRCC sarcomatoid renal cell carcinomaThe most common pseudotumours are hypertrophic columns and fetal lobulation, which are quite common. These two conditions can mimic a solid lesion, especially for less experienced radiologists. Hypertrophic columns will appear on B-mode US as nodular lesions protruding into the renal sinus. Doppler can help in these cases by distinguishing between solid malignant lesions and anatomical variants as there is no distortion of the renal vascular architecture on Doppler, though making such distinctions requires radiological expertise. CEUS, however, is more immediate because it shows that the enhancement of these nodules is identical to that of the surrounding parenchyma. The high capacity of CEUS to detect enhancement, even for small lesions, makes it an excellent method for identifying contrast in suspicious lesions with pseudo-enhancement on CT [1, 10] (Figs. 1, 2, 3, 4, 5).
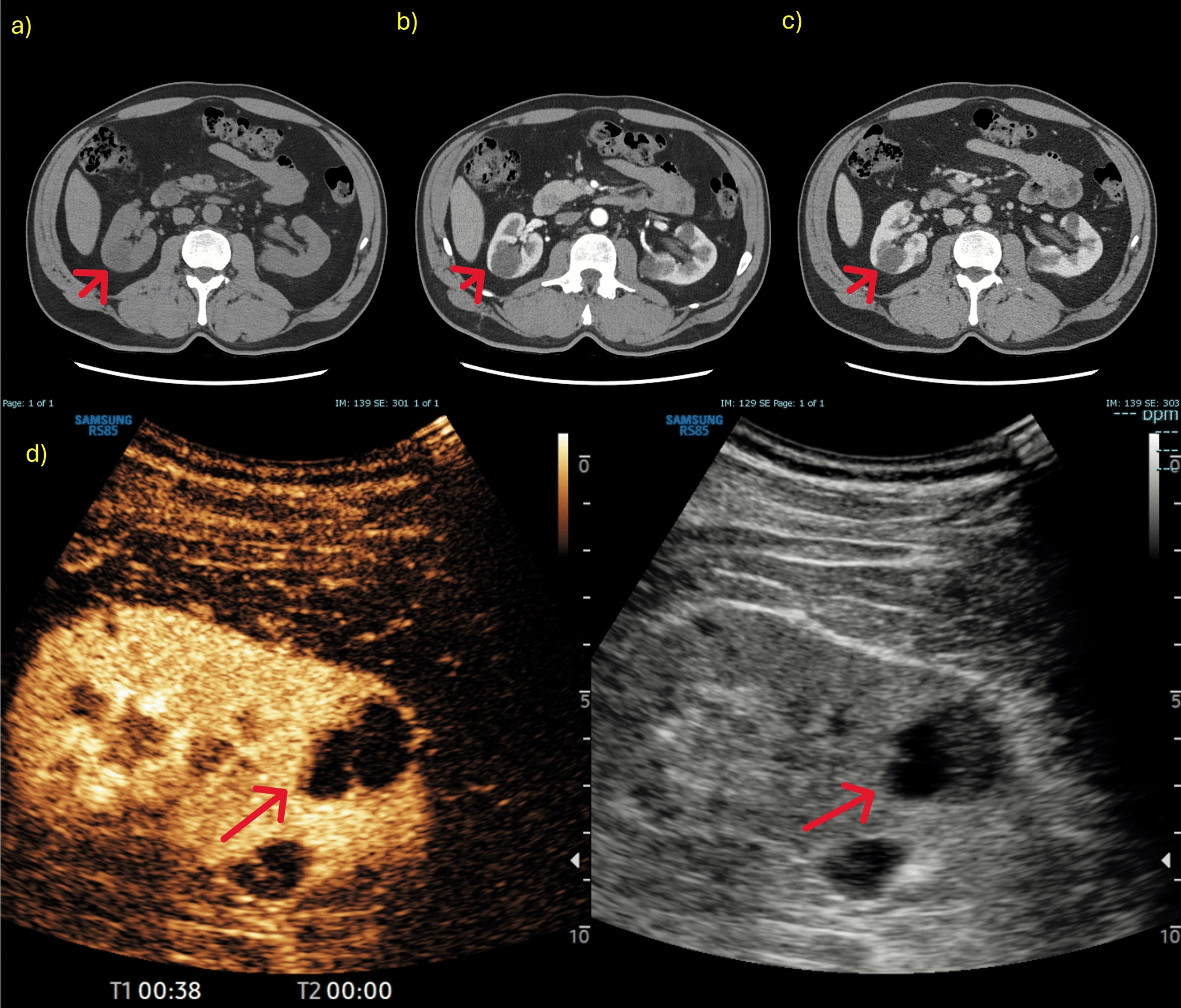
Fig. 1
a-d CT images of a right renal lesion (red arrow) that appeared hypodense in the basal phase (a) but seemed to show a pseudo-enhancement in the parenchymal (b) and nephrographic (c) phases. CEUS evaluation (d) confirmed a non-contrast enhancing lesion; US images were obtained with the patient lying supine
Fig. 2
a, b A case of indeterminate lesion. US images of a renal evaluation in B-mode (a) showed a hypo-isoechoic formation (red arrow) in the right renal lower pole, confirmed on CEUS (b) as a renal mass with homogeneous contrast enhancement; US images were obtained with the patient lying supine
Fig. 3
a, b A case of pseudotumour. US images of a renal evaluation in B-mode (a) showed a bumpy and pseudo-nodular appearance of the cortical region of the renal middle third. CEUS examination (b) revealed no pathological enhancement with findings attributable to a prominent column of Bertin. US images were obtained with the patient lying supine
Fig. 4
A case of a vascular lesion. CEUS showed focal acute cortical ischemia (curved arrows) and patent interlobar vessels (arrowheads). *Image source: Granata A, Campo I, Lentini P, Pesce F, Gesualdo L, Basile A, et al. Role of Contrast-Enhanced Ultrasound (CEUS) in Native Kidney Pathology: Limits and Fields of Action. Diagnostics. 2021 Jun 8;11(6):1058. This is an open access article distributed under the terms of the Creative Commons Attribution (CC BY) 4.0 license. (http://creativecommons.org/licenses/by/4.0/)
Fig. 5
a-f A case of a vascular lesion. NECT images (a) showed a parenchymal hyper-density from a recent hematoma (arrowhead) at the lower pole of the left kidney. CECT images showed a pseudoaneurysm (curved arrow) in the arterial phase (b); while in the nephrographic phase (c) the parenchymal contusion is more clearly recognized and the pseudoaneurysm is less visible. B-mode US (d) showed inhomogeneous echogenic areas (asterisks) corresponding to the contusions; CEUS (e) adequately showed all the vascular phases of the pseudoaneurysm (curved arrow) and the perirenal hematoma (asterisk); CEUS follow-up performed on 7th day (f). *Image source: Granata A, Campo I, Lentini P, Pesce F, Gesualdo L, Basile A, et al. Role of Contrast-Enhanced Ultrasound (CEUS) in Native Kidney Pathology: Limits and Fields of Action. Diagnostics. 2021 Jun 8;11(6):1058. This is an open access article distributed under the terms of the Creative Commons Attribution (CC BY) 4.0 license. (http://creativecommons.org/licenses/by/4.0/)
Follow-up of renal lesions under active surveillanceThis is another indication for CEUS according to EFSUMB guidelines. Most renal lesions are detected incidentally during exams performed for other reasons, and this incidental detection has exponentially increased over the past few decades [1, 10]. Renal cancer was previously considered the internist's tumour, presenting as a palpable mass, flank pain, and haematuria, but it is now seen as the radiologist's tumour as we are responsible for most initial diagnoses. More frequently, we are detecting small renal masses (less than 4 cm), which are benign in 25% of cases and aggressive lesions (renal cell carcinoma, RCC) in 10%, with a metastasis risk below 2%. The likelihood of benignity increases as the mass size decreases [11,12,13]. More often, these lesions are found in elderly patients over seventy with comorbidities, raising issues regarding differential diagnosis and patient management. Once a lesion is detected, the patient must be directed to a diagnostic and therapeutic pathway. For all these reasons, over the past 10 years there has been growing advocacy for active surveillance rather than immediate surgical intervention for these small renal lesions. Active surveillance involves monitoring tumour size through imaging (US, CT, or MRI). Active surveillance differs from watchful waiting, which is reserved for patients whose comorbidities contraindicate any further active treatment and do not require imaging monitoring unless clinically indicated [14]. However, there are currently no specific guidelines regarding the timing of active surveillance or the methods to be used, though a method with low biological and economic cost should be employed. The EAU guidelines state that the lesions to be subjected to active surveillance are numerous as they represent the majority of those detected daily (Table 2). Given these challenges, the role of CEUS in the follow-up of small renal masses has gained increasing attention. CEUS provides real-time dynamic assessment of lesion enhancement, which is crucial for differentiating between benign and malignant renal masses. Lesions that show homogeneous hyperenhancement with slow washout are often indicative of benign conditions, such as oncocytomas or angiomyolipomas, making them suitable for active surveillance. Conversely, lesions demonstrating rapid washout, rim-like enhancement, or irregular vascularization raise suspicion for RCC and may necessitate early therapeutic intervention. In addition, CEUS has proven valuable in assessing lesion perfusion over time. For example, a growing but persistently hypo-enhancing lesion with minimal vascularity may suggest a low-grade tumour with indolent behaviour, supporting continued surveillance. On the other hand, the development of necrotic areas or increasing vascular heterogeneity could signal tumour progression, prompting the need for biopsy or definitive treatment. Given its ability to detect subtle perfusion changes, integrating CEUS into active surveillance protocols may improve risk stratification and clinical decision-making. The ACR has included CEUS as a suitable method for the follow-up of lesions under active surveillance, with appropriateness comparable to CT or MRI, as it is a method free from ionizing radiation, uses a non-nephrotoxic contrast agent, and is also cost-effective. Recent studies such as that of Aaron Oh et al. have demonstrated that CEUS is more cost-effective than traditional imaging techniques such as CT or MRI in the active surveillance of Bosniak III and IIF complex renal masses [15].
Table 2 Factors influencing active surveillance of renal lesionsCharacterization of indeterminate lesions in patients with transplanted kidneysThese patients are inherently nephropathic as they have only one functioning kidney, and they often reject iodinated contrast agents due to the fear of side effects, particularly those associated with renal excretion. CEUS, having pulmonary excretion, is extremely valuable in this context.
When evaluating the transplanted kidney, it is equally important to assess the native kidney of the transplanted patient. Especially in patients who underwent dialysis prior to transplantation, native kidneys are prone to a condition called acquired cystic kidney disease (ACKD), which increases the risk of developing renal cancer by 19% compared to the general population. Thus, it is crucial to implement surveillance, particularly of the native kidney, which is often done with US alone [6]. If CEUS raises the suspicion of a renal lesion, the patient should be referred for CT or MRI, especially to guide surgical planning. In the case of equivocal lesions on B-mode US, it is advisable to perform CEUS to determine whether the lesion is vascularized or not. If the lesion is not vascularized, the patient may avoid undergoing a CT scan that uses nephrotoxic contrast agents.
Inflammatory-infectious pathologiesAmong the indications for CEUS are inflammatory-infectious pathologies, such as pyelonephritis. CEUS can detect the presence of acute pyelonephritis, which appears as areas of poorly vascularized parenchyma. In the acute phase, these areas tend to have a more rounded shape, but over time, they acquire a triangular morphology. Renal abscesses are also easily visible on CEUS, even when small in size, presenting as rounded lesions without contrast enhancement, sometimes with a rim of perilesional enhancement. The diagnostic accuracy of CEUS appears to be lower in cases of diffuse pyelonephritis due to the inability to simultaneously compare both kidneys. However, in focal and multifocal forms, authors have reported significant diagnostic accuracy, with a positive predictive value of 100% and a negative predictive value of 89%, though this was observed in a selected population with a high probability of disease [16, 17]. In addition to diagnosis, CEUS is important for monitoring the evolution of abscessed lesions. It allows for detailed measurement of lesion size and, more importantly, the precise differentiation between liquefied and peripheral areas. Focal pyelonephritis often appears on gray-scale US as a focal hyperechoic lesion with cortical swelling. The hyper-echogenicity on B-mode is due to numerous interfaces correlated with abundant inflammatory cells in the interstitium and tubules. In addition to the inflammatory infiltrate and edema, severe capillary damage has been demonstrated, with the presence of intraluminal leukocytes and fibrin plugs. These pathological findings correlate with the hypo-echogenic appearance on CEUS and the reduced enhancement of these lesions compared to the surrounding cortex. Areas of focal pyelonephritis are more visible during the late parenchymal phase as these wedge-shaped or rounded areas appear more hypo-echogenic during this phase. Abscesses appear as heterogeneous or hypo-echogenic focal lesions with cortical swelling. CEUS can be used to assess the size, internal structure, and extent of abscesses. An abscess is a necrotic cavity containing pus and debris that does not exhibit enhancement during any phase. Conversely, enhancement of the septa can be seen if the abscess is partially liquefied. Enhancement of the peripheral rim can also be observed during the cortical phase. Focal pyelonephritis and abscesses of various sizes appear in different phases of CEUS. Abscesses are characterized by a rounded shape and an anechoic structure on B-mode. They are completely avascular in all post-contrast phases and may have a thin rim of enhancement. Areas of pyelonephritis are generally located in the cortical region and are typically isoechoic or hyperechoic on B-mode, wedge-shaped, and appear hypo-vascular after contrast injection. They are more evident during the late parenchymal phase (Fig. 6).
Fig. 6
a-c A case of complicated pyelonephritis. US images of a renal evaluation in B-mode (a) showed an inhomogeneous, hypoechoic area (asterisk). CEUS (b) confirmed the presence of an avascular lesion with a peripheral rim, consistent with abscess (asterisk). Urographic phase CECT (c) confirmed the presence of the abscess (asterisk) and of a hypo-perfused area (curved arrow) at the lower pole of the kidney. *Image source: Granata A, Campo I, Lentini P, Pesce F, Gesualdo L, Basile A, et al. Role of Contrast-Enhanced Ultrasound (CEUS) in Native Kidney Pathology: Limits and Fields of Action. Diagnostics. 2021 Jun 8;11(6):1058. This is an open access article distributed under the terms of the Creative Commons Attribution (CC BY) 4.0 license. (http://creativecommons.org/licenses/by/4.0/)
Additional roles of CEUS in solid mass lesion evaluationOne of the indications from EFSUMB guidelines includes the study of advanced renal lesions to evaluate caval thrombosis, not just the renal lesion itself. Studies have demonstrated the efficacy of CEUS in assessing thrombosis, distinguishing between neoplastic and non-neoplastic thrombi [18, 19]. CEUS is useful for determining whether a thrombus shows post-contrast enhancement, which is critical information for surgeons when deciding if the thrombus is a red thrombus or a neoplastic thrombus. If it is a neoplastic thrombus, it will exhibit contrast enhancement. Another important application of CEUS, as outlined by EFSUMB guidelines, is the evaluation of solid lesions that may develop in the surgical bed following nephrectomy. Studies have provided evidence of CEUS aiding in the differentiation of recurrent tumours from post-surgical fibrosis. This differentiation is crucial for guiding further treatment decisions, including the need for additional surgical intervention or targeted therapy [20].
Comments (0)