Delayed diagnosis of autism and psychiatric and/or neurodevelopmental co-occurring conditions
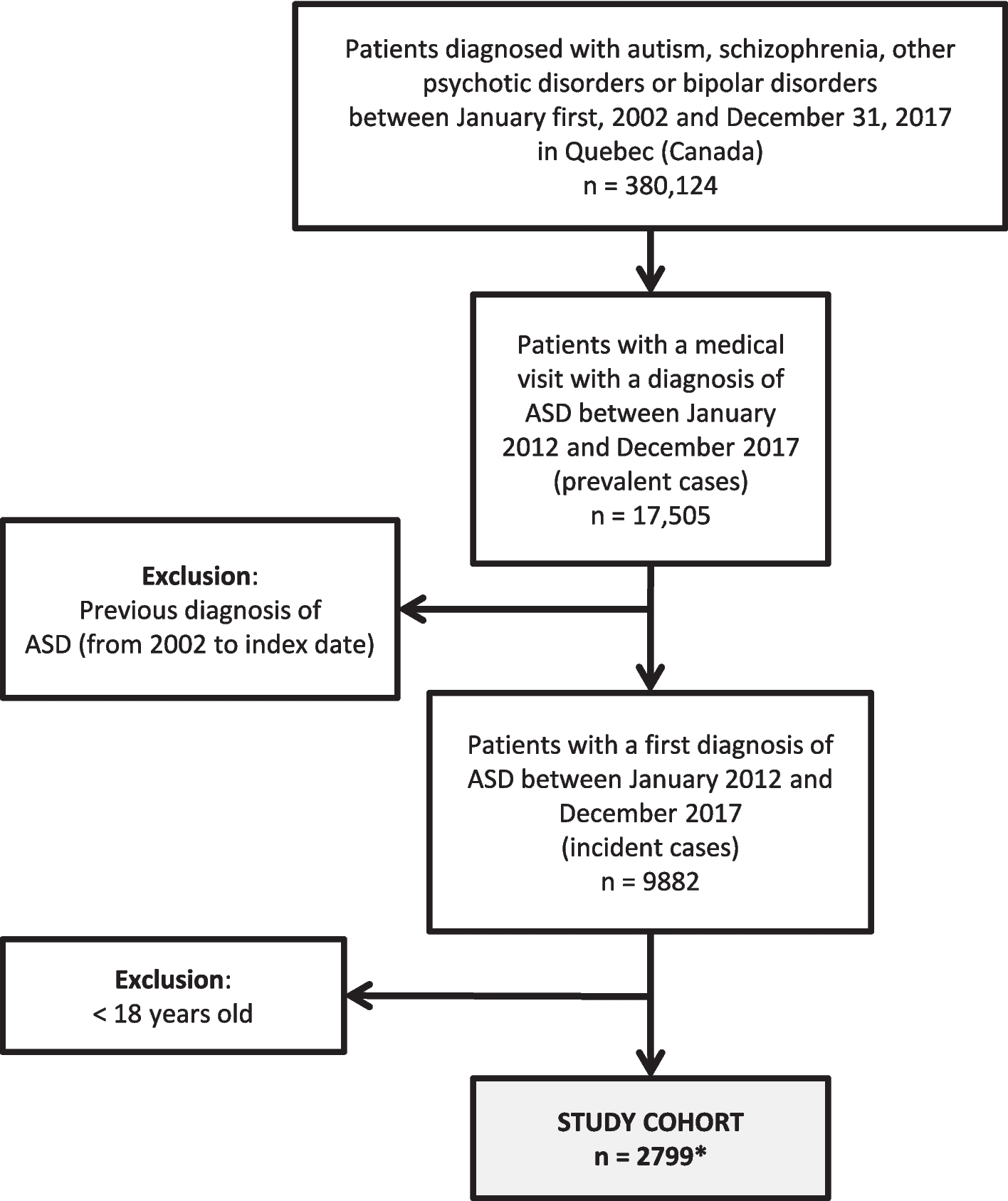
In line with previous studies, in our study, up to 28% of the individuals diagnosed for the first time between 2012 and 2017 were adults; the male-to-female ratio was 2:1, with half of the cohort receiving a first autism diagnosis at 36 years old and older (Fig. 1, Table 1) [1, 9].
Many factors can contribute to delayed diagnoses. A key factor is the age distribution of the study cohort: the median age of 36 years indicates that more than half of the individuals were born in 1981 or earlier, a period when autism was first recognized with the release of the DSM-III in 1980 and the ICD-9, adopted for administrative databases in Quebec in 1979 [1, 3, 8]. Consequently, most adults in the study cohort came of age at a time when signs of autism in children without IDDs were often overlooked, misdiagnosed, or never referred to mental health services. The expansion of diagnostic criteria toward a broader spectrum approach in the DSM-5 (2013) and the rise in community awareness have led to an increase in autism assessments [5, 9].
Other important reasons for delayed diagnoses have been proposed. Autistic individuals with more pronounced forms of autism are more likely to have been diagnosed in childhood, while those without IDDs and requiring lower levels of support may not face significant challenges until adulthood [2, 4, 15, 25]. A hypothesis suggesting a potential contributing cause of missed or delayed diagnoses is that the use of coping or camouflaging strategies (especially among females) may obscure the detection of autistic symptoms [4, 9, 17, 18], although questions have arisen in recent years regarding the foundations of this hypothesis [51, 52]. Several studies also suggest that females tend to exhibit less severe social communication challenges and fewer repetitive or stereotyped behaviors [6, 24]. That being said, many autistic individuals have reported poor past experiences with mental health services, prolonged treatments, and long waiting times, before obtaining an assessment for autism [4, 9, 10, 15].
As expected, most individuals in this study cohort were diagnosed with several psychiatric and/or neurodevelopmental conditions. IDDs, ADHD, and OCD fall within the range of pooled prevalences of recent meta-analyses on neurodevelopmental co-occurring conditions associated with autism [20,21,22, 27, 53]. However, the cohort's prevalence of anxiety, depressive and personality disorders, as well as SSD and bipolar disorder appears notably high compared to previous meta-analyses. However, an umbrella review [20] reported wide prevalence ranges for SSD (4–67%), depression (2.5–47.1%), bipolar disorder (4.4–37%), and anxiety (2.5–47.1%). Personality disorder prevalence varies from 6–12.6% [21, 54, 55], though rates of up to 60% in autistic adults have been reported [15]. Study design differences and reliance on health administrative data may contribute to overrepresentation of psychiatric conditions. In addition, the algorithm used to identify co-occurring conditions, based on at least one recorded diagnosis (favoured sensitivity over specificity), may overestimate prevalence. Nonetheless, a closer examination of the longitudinal patterns of diagnoses in the sequence index plots (Fig. 2b) supports the reliability of these conditions. For instance, repeated diagnoses of anxiety and neurodevelopmental conditions in Type 3, SSD in Type 4, and bipolar disorder in Type 5 suggest that reported rates reflect valid and often long-lasting conditions.
Trajectories of diagnoses
Results from the state sequence analysis (SSA), a data-driven approach based on diagnoses received during MHC use over time, revealed highly variable pathways to autism diagnosis in adulthood. Five distinct types of TDs emerged (Figs. 2 and 3). The TDs Types 1 and 2, shared by the majority of the cohort (63.8% and 17.6%, respectively), exhibit similar individual characteristics, but very different sequences of psychiatric and/or neurodevelopmental diagnoses over time.
Types 1 and 2 also indicate that, before the increase in MHC seeking, anxiety disorders were likely predominant from adolescence or early adulthood, given the younger age groups in these types. It can be hypothesized that these types represent autistic individuals facing challenges of living with autism, resulting in additional disturbances [2, 4, 11, 32]. Several studies indicate that anxiety disorders are amongst the most common co-occurring conditions in youth with autism. Also, youth are estimated to frequently experience clinically significant anxiety symptoms in the range of 40 to 69%, commonly involving specific phobias, OCD, and social anxiety disorder, especially in those with IDDs [56,57,58,59,60,61]. Several hypotheses could explain the relatively low prior MHC use in Type 1. First, it is well established that many individuals with mental health conditions do not seek care, particularly younger individuals and males. Importantly, despite lower MHC use compared to other types, over 50% and 71% of individuals in Type 1 received at least one diagnosis of depression and anxiety, respectively, and more than 20% had a diagnosis of ADHD. Second, many may have initially sought care for physical health concerns, which frequently co-occur with autism and neurodevelopmental conditions. Nearly half of the index autism diagnoses in this group occurred during hospitalization, and only 48% of those hospitalizations were associated with mental, behavioral, and neurodevelopmental disorders, substantially lower than in other types. Nonetheless, over 63% of individuals in this group received three or more autism diagnoses over the study period, indicating subsequent referral and diagnostic confirmation. Upon closer examination of sequences of MHC use in Type 1, there is no noticeable change in healthcare-seeking patterns over time, except for autism. Conversely, in Type 2, after a peak around the index date, there is a decreasing trend in MHC use associated with other diagnoses alongside the autism diagnosis, except for SSD (affecting 60% of individuals). Studies have reported that individuals with intellectual disabilities are at an elevated risk of developing anxiety, mood, and psychotic disorders, which also frequently co-occurs with anxiety disorders [27, 62,63,64].
Type 3, representing 6% of the cohort, exhibits individual characteristics that barely differ from those in types 1 and 2 (Table 1), except for neurodevelopmental diagnoses, particularly IDDs (53.9%), ADHD (33.5%), OCD (13.8%), and Tourette syndrome (10.2%). Notably, members of Type 3 have likely experienced a prolonged history of high MHC use associated with anxiety disorders, ADHD and depressive disorders since childhood and adolescence, conditions known to frequently co-occur with autism [31, 32, 57]. The differential diagnosis of anxiety, depression or other conditions can be particularly challenging in individuals with IDDs, who may struggle to articulate their experiences, often resulting in misdiagnoses [9, 31, 56]. With the exception of IDDs, healthcare seeking gradually decreased alongside the initial diagnosis of autism. It can be hypothesized that once accurately diagnosed, autistic adults with IDDs in Type 3 may benefit from more tailored support and services.
Two additional distinct trajectories emerged from the SSA: Type 4 (9%), with a predominance of SSD, and Type 5 (3.6%), with a predominance of bipolar disorder, with about half of the individuals being female. Both types represent middle-aged to older individuals, with a median age of around 50 years at the index date. The co-occurrence of these disorders with autism is well-documented, with an increased prevalence of schizophrenia/psychotic disorders in males, and bipolar disorder in females [20, 22, 53, 65].
Although distinct conditions, autism, schizophrenia/psychotic, and bipolar disorders share overlapping clinical features, genetic patterns, and etiological risk factors, which could complicate differential diagnosis and delay the recognition of autism [26, 27, 53,54,55, 66, 67]. Clinicians may also prioritize early detection and intervention for psychotic and bipolar disorders, due to the potential impact of outcomes. For example, early detection of a first episode of psychosis is crucial for initiating appropriate treatment and significantly influences prognosis. However, distinguishing psychotic symptoms from non-psychotic conditions such as autism, which may present with similar features, can pose major challenges, even for expert clinicians [27, 68, 69]. Conditions requiring timely intervention, such as schizophrenia/psychotic and bipolar disorders, as well as major depressive disorder, might contribute to the delayed diagnosis of autism observed in Types 4 and 5 compared to other trajectories.
Beyond the influence of co-occurring SSD/psychotic and bipolar conditions in Types 4 and 5, the median age of 50 years signifies that more than half of these individuals were born in 1973 or earlier, well before the initial recognition of autism in the DSM-III. As a result, some of these adults may be regarded as a "lost generation" with a missed opportunity for autism assessment [15]. However, it is worth noting that 44–51% of patients in these types had only a single registered autism diagnosis, made later in life and despite a history of extensive mental healthcare use. This raises concerns about the validity of autism diagnoses among middle-aged adults with SSD or chronic psychotic and bipolar conditions. When autism is suspected, Quebec and Canadian guidelines (since 2012) recommend a comprehensive assessment involving medical history, physical examination, and developmental and behavioral evaluations [70,71,72]. For individuals with complex psychiatric profiles, diagnosing autism at a later age could reflect changes in diagnostic criteria, or represent"last resort"diagnoses of suspected autism, with referrals for comprehensive diagnostic assessment. However, these suspected diagnoses may not have been confirmed later [60, 73]. It is also notable that, across the five types of TDs, the proportion of individuals with only a single recorded ASD diagnosis, or potentially unconfirmed cases, tends to increase with age. These findings suggest possible overdiagnosis in middle-aged and older adults, particularly when presenting with a long history of SSD/psychotic or bipolar disorders and when developmental history is lacking. Prior research has shown that requiring multiple ASD diagnoses in administrative data improves the algorithm's specificity and positive predictive value, although it reduces its sensitivity [74,75,76].
Differential diagnosis, misdiagnosis and overdiagnosis
Accurate diagnosis is incredibly challenging for clinicians, who often face difficult diagnostic differentiations within pressured or time-constrained contexts. Although expanded diagnostic criteria have increased sensitivity, especially for older adults without cognitive impairment, the ambiguous and heterogeneous phenotypic presentation of the autism spectrum, along with characteristics overlap with other neurodevelopmental or psychiatric conditions complicates the process, often resulting in misdiagnoses, delayed, or missed diagnoses of autism [4, 15, 23, 26, 27, 33, 77, 78]. Additionally, in clinical practice, assessment tools are often limited to a single diagnosis, making it challenging to evaluate co-occurring conditions. For example, the Autism Diagnostic Observation Schedule (ADOS) and the Autism Diagnostic Interview-Revised (ADI-R), widely used for diagnosing autism, focus solely on autism-specific traits and behaviors, overlooking co-occurring conditions. Furthermore, for older adults and women, more subtle or masked presentations of autism are frequently missed. This underscores the need for accurate diagnosis, comprehensive care, and treatments to address the full spectrum of needs in autistic individuals with co-occurring conditions [19, 23, 79,80,81].
Diagnostic overshadowing, particularly in autistic adults requiring minimal support, occurs when prominent symptoms of co-occurring psychiatric disorders, such as SSD/psychotic disorders, bipolar disorder, major depressive disorder, and personality disorder, mask signs of autism [16, 24,





Comments (0)