The single-center cross-sectional study was conducted at the second affiliated hospital of Baotou Medical College, Inner Mongolia University of Science and Technology. This study was approved by the Institutional Review Board of the Second Affiliated Hospital of Baotou Medical College (review number LW-022) and complies with the Declaration of Helsinki. All participants signed a written consent.
This study included patients older than 18 years old and diagnosed with dry eye between February 2022 and December 2022. The diagnosis was based on the TFOS DEWS II[5]. The diagnostic process included the following specific methods:
(1)
Symptom Assessment: A validated Ocular Surface Disease Index (OSDI) questionnaire in Chinese version was used to assess the perceived symptoms and quality of life with the score ranging from 0(no symptom) to 100(severe symptoms)[9]. A positive symptom score (≥ 13 points) prompted further diagnostic testing.
(2)
Ocular Surface Staining: Fluorescein sodium was used to stain the cornea and conjunctiva to identify superficial punctate epithelial erosions. The staining was observed through a cobalt-blue filter and graded from 0 to 15 using the National Eye Institute/Industry (NEI) scale [10]. The sum of scores from five corneal sections was graded as follows: 0 = normal (no staining), 1 = mild (< 10 scattered dots), 2 = moderate (10–30 dots), and 3 = severe (> 30 dots, confluent staining, or corneal filaments), with higher scores indicating more severe dry eye.
(3)
Tear break-up time (TBUT): TBUT was measured using fluorescein sodium to assess tear film stability. A TBUT of less than 10 s was considered indicative of dry eye.
(4)
Meibomian Gland Dysfunction (MGD) Assessment: Biomicroscopic examination of the meibomian glands was performed to evaluate gland morphology, expressibility of secretions, and the quality of meibum. This assessment helped identify evaporative dry eye associated with MGD.
The study excluded patients who had experienced ocular injury, infection, allergic conjunctivitis, or undergone surgery in the past six months. Additionally, individuals with systemic autoimmune conditions, including Sjogren’s syndrome and systemic lupus erythematosus, were also excluded from the study. Patients were diagnosed with type 2 diabetes in accordance with the criteria established by the American Diabetes Association [6]. The following data was recorded: age, gender, history, and type of diabetes, and fasting blood glucose levels were tested at the same time point in all patients. Ocular surface examinations were conducted to assess the tear film stability, morphology and physiological function of lid margin and meibomian glands. Clinical tests were performed from the least to the most invasive, and the outcomes were recorded.
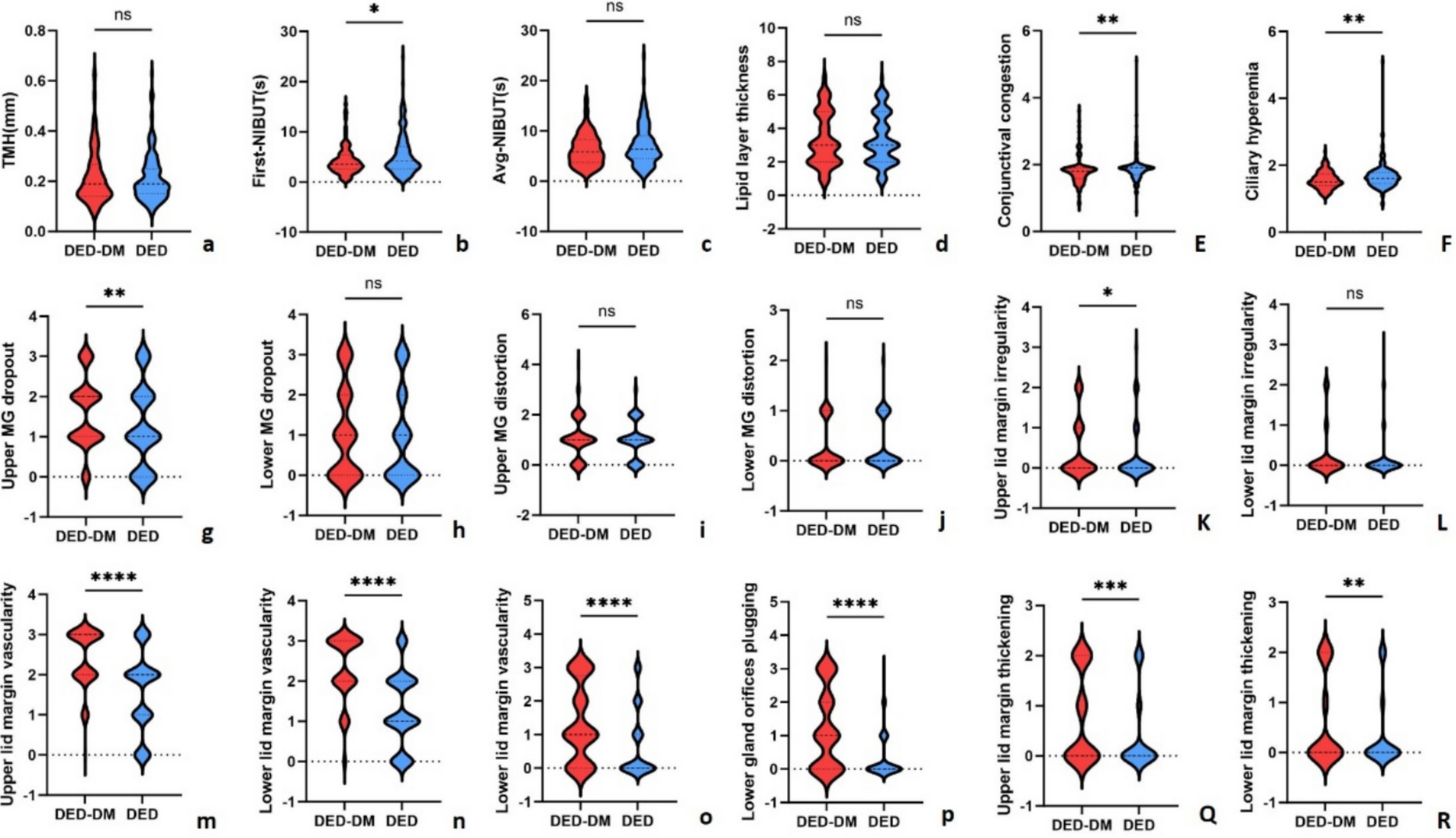
Non-invasive tear breakup time (NIBUT) and tear meniscus height (TMH)
The NIBUT and TMH were tested with an Oculus Keratograph 5 M (K5M; Oculus Optikgeräte GmbH, Wetzlar, Germany). Participants rested their chin on the chin rest with their foreheads pressed against the forehead band and watched a fixed pattern without blinking. The tear breakup time was examined automatically and the first and average tear breakup time was reported [11]. The TMH was measured by K5M for consecutive 3 times, and the mean value was recorded [11].
First tear breakup location
The tear film assessment software divides the 360° ocular surface into 24 bands (15° for each band), then subdivides each band into eight small rectangles, each of which serves as a basic break-up unit. The color of the unit in a certain location represents the TBUT of this unit, which changes in color from red to yellow to green as the TBUT increases. In the present study, the entire 360° precorneal surface was divided into 4 quarters of 90° each. The domain of each first break-up unit was recorded [12].
Conjunctival congestion and ciliary hyperemia
K5M was used for quantitative analysis of conjunctival congestion and ciliary hyperemia automatedly. Automatic analysis of the comprehensive redness level of both conjunctival congestion and ciliary hyperemia: 0–1 indicates normal eye redness, 2 indicates mild eye redness, 3 indicates moderate eye redness, and 4 indicates severe eye redness. A level greater than 2 indicates an abnormality.
Lipid layer thickness
The LipiView Interferometer (TearScience Inc., Morrisville, NC, USA) was used to measure the tear film lipid layer thickness (LLT). Patients were instructed to look straight ahead with both eyes and blink normally. The measurement was completed within 20 s.
Grading of meibography images
Infrared meibography images were taken using the K5M device. Researchers opened the eyelids to fully expose the conjunctiva, ensuring reliable image capture for assessing meibomian gland conditions, including the extent of gland dropout and morphological changes. Meibomian gland (MG) dropout was categorized as follows: 0 = 0–25% loss; 1 = 26–50% loss; 2 = 51–75% loss; 3 = 76–100% loss [13]. MG distortion was rated on a scale of 0 to 5: 0 = no distortion; 1 = distortion > 90°, area < 1/3; 2 = distortion > 90°, area 1/3–2/3 or distortion 45–90°, area < 1/3; 3 = distortion > 90°, area > 2/3 or distortion 45–90°, area 1/3–2/3; 4 = distortion 45–90°, area > 2/3 or distortion 45°, area < 50%; 5 = distortion < 45°, area > 50%.[14].
Grading of lid margin images
Lid margin images were obtained using a slit lamp (10 × magnification) equipped with a camera under diffuse illumination. Two researchers graded lid images based on the protocol introduced by Arita and associates [15]. The discrepancy between the two researchers was discussed with another researcher.
Plugging of gland orifices was graded from 0 to 3: 0 = no plugging of gland orifices; 1 = fewer than three pluggings of gland orifices; 2 = three or more pluggings of gland orifices with a distribution of less than half of the full length of the lid; 3 = three or more pluggings of gland orifices with a distribution of half or more of the full length of the lid.
Vascularity was graded from 0 to 3: 0 = no or slight redness in lid margin conjunctiva and no telangiectasia crossing meibomian gland orifices; 1 = redness in lid margin conjunctiva and no telangiectasia crossing meibomian gland orifices; 2 = redness in lid margin conjunctiva and telangiectasia crossing meibomian gland orifices with a distribution of less than half of the full length of the lid; 3 = redness in lid margin conjunctiva and telangiectasia crossing meibomian gland orifices with a distribution of half or more of the full length of the lid.
Irregular lid margin was graded from 0 to 2: 0 = no lid margin irregularity; 1 = fewer than 3 lid margin irregularities with shallow notching; 2 = three or more lid margin irregularities or deep notching.
Lid margin thickening was graded from 0 to 2: 0 = no lid margin thickening; 1 = lid margin thickening with or without localized rounding; 2 = lid margin thickening with diffuse rounding.



Comments (0)