Intravitreal anti-VEGF therapy is the primary treatment for wet AMD. Since their clinical introduction, various studies have examined the optimal treatment regimens and injection frequencies, often with strict exclusion criteria. Our study aimed to provide real-life data for nAMD patients treated and monitored for approximately 10 years.
In our study, the average initial vision was 59.0 ± 18.3 letters, after 3 loading injections, there was an average gain of 10.8 letters, which was maintained for the first 2 years. There are many short-term randomized controlled studies in the literature which showed similar results [5, 11, 12]. In the SEVEN-UP study, which is a continuation of the ANCHOR, MARINA, and HORIZON studies, when the final vision was evaluated after an average of 7.3 years, a loss of 8.6 letters compared to the beginning and a loss of 22 letters compared to the 2nd year of treatment was observed, and their number of injections per year was 1.6 for 4 to 7 years [13]. Although intravitreal anti-VEGF treatment may not sustain first-year success, it preserves vision better than the natural progression of the disease [14]. In our study, visual acuity decreased gradually over the following years. At the end of 10 years, the average BCVA was 60.4 ± 17.5, the initial vision level was preserved, and there was a gain of 1.4 letters, but the 11-letter gain after loading treatment, which was maintained for 2 years, was significantly lost.
Spooner et al. in their LATAR study, showed a gain of 3 letters after 10 years of follow-up with the modified TE regimen, In the 'The Fight Retinal Blindness!' (FRB) project, there was a gain of three letters at the end of 10 years of follow-up with the modified TE regimen and a loss of 0.9 letters in both the PRN and TE groups. There was a loss of five letters in patients who were followed for 10 years with the PRN regimen in the study conducted by Brynskov et al., and the Moorsfields group reported that there was a loss of 2.1 letters in patients who were initially treated with the PRN regimen followed by TE [8, 15,16,17]. These results are similar to those of our study and show that vision levels can be preserved after 10 years. In the study conducted by Peden et al., at the end of 7 years of follow-up, they achieved a gain of 12.1 letters with an average of 10.5 injections per year, while Adrean et al. reported a gain of 8.7 letters in patients followed for an average of 8 years who had 50 or more injections during their follow-up [18, 19]. A common feature of these two studies was the high average number of injections per year. While Peden et al. had been following their patients on monthly fixed doses, Adrean et al. practice the treat-extend-stop (TES) protocol. These studies indicates that the treat-and-extend approach may yield improved visual acuity outcomes and enhanced disease management, involving more injections administered during fewer clinical visits. Nevertheless, the research conducted by Peden et al. and Adrean et al. reported mean baseline VA scores of 45.6 and 55.6 letters, respectively, which are 14 and 4 letters lower than our study's findings. As a result, their study participants might have had a greater opportunity for improvement. Many studies on treatment regimens have been published, with variable results. Pro-re-nata (PRN), a primary treatment regimen, has been effective for years. Essentially, it involves administering treatment during follow-up as needed after a 3-month loading dose. Regimens like treat-and-extend and treat-extend-stop are commonly used and yield results comparable to fixed monthly treatments [19].
In our study, there was no significant difference in the number of injections between the increasing, decreasing, and stable groups (p = 0.673). The variables that were found to be significantly different were age (p = 0.018), baseline BCVA (p = 0.001), previous PDT treatment (p = 0.025), and detection of submacular hemorrhage(p = 0.049).
The mean age of the patients in the stable group was significantly lower than those in the decreasing and increasing groups (p = 0.005). Brynskov et al., Spooner et al., and SEVEN-UP found that the mean age was significantly lower in patients with increasing vision. In contrast, the Moorfields group did not show a significant difference in age [13, 15,16,17].
A statistically significant difference was found in the baseline BCVA values between the decreasing, stable, and increasing groups (p = 0.001). There were more patients in the decreasing group with > 60 letters at the initial examination than in the stable and increasing groups. Despite a more frequent decline in vision among patients with higher initial visual acuity, their final vision was superior (p < 0.001). This phenomenon, known as the ceiling effect, has been well-documented in the literature. Brynskov et al. and Westborg et al. reported that patients with low initial vision experienced greater gains, although the ceiling effect was less pronounced in the Danish group [17, 20]. Conversely, the Moorfields group found that patients with letter gains had better initial visual acuity. They noted that patients starting with 52 letters or fewer had limited improvement potential, likely because of the underlying irreversible retinal damage [16].
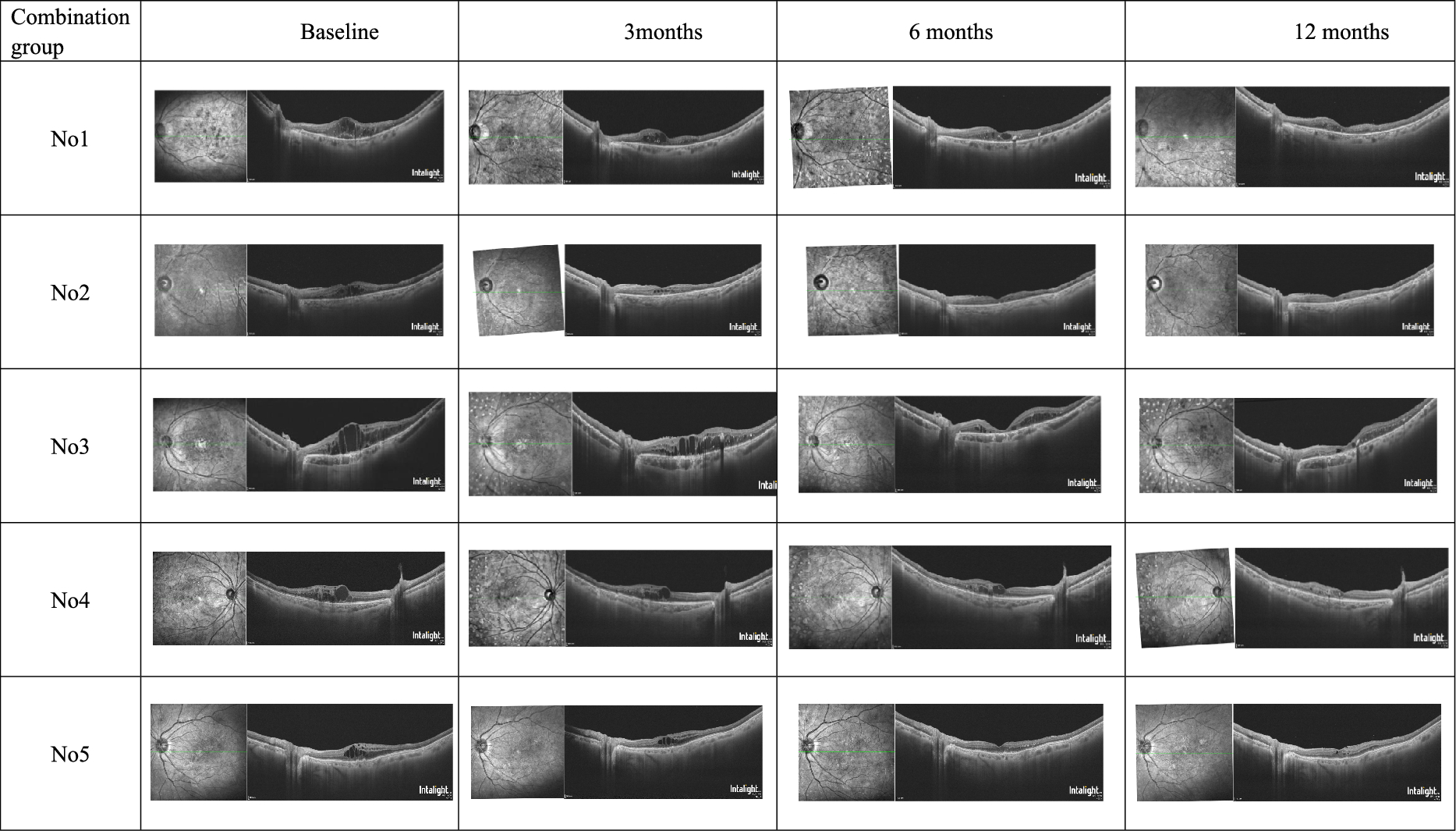
According to the groups, there was a statistically significant difference between receiving anti-VEGF treatment alone or in combination with PDT (p < 0.05). The proportion of PDT patients in the stable group was higher than in the decreasing group. However, the final VA of PDT patients did not differ significantly from the other group (p > 0.05). The efficacy of PDT in treating MNV has been previously demonstrated; however, with the advent of anti-VEGF therapy, PDT has been superseded in AMD patients, although it retains importance in PCV treatment in conjunction with anti-VEGF therapy [21, 22]. Nevertheless, selective occlusion of choroidal vessels by PDT may contribute to maintaining stable VA in AMD patients in our study.
This study coincided with the COVID-19 pandemic, complicating hospital access for many patients, particularly those over 65 years of age. Despite various precautions in our clinic to minimize the impact, some treatments were interrupted. A total of 22 eyes experienced a treatment interruption lasting between 1 and 1.5 years. Among the 6 eyes that underwent a break without receiving any treatment, there was a significant visual deterioration, with a loss of 3 to 6 lines of vision compared to the pre-pandemic examination, and vision decreased to below 20/200. However, upon separate evaluation, no statistically significant difference in final vision was observed (p = 0.95). This may be attributed to fibrosis or atrophy that develops during the natural progression of the disease despite treatment.
When the patients' vision levels at the last examination were examined, 24 eyes (24%) were below 20/200, 37 eyes (36%) were between 20/200 and 20/40, and 41 eyes (40%) were above 20/40 according to the Snellen chart. After an average of 10 years, 76% of our participants were self-sufficient, while 40% had sufficient vision to drive in many countries. In the Moorfields group, 67.1% of the patients were above 20/70, 33.5% had a final vision level above 20/40, and 14% were below 20/200. In the SEVEN-UP study, one-third of the patients were above 20/70, while a quarter were above 20/40 [13, 16]. Similar rates have been observed in studies categorized according to vision level; however, the disease remains active in many patients. In our study, after an average of 10 years, MNV had become inactive (fibrotic or atrophic scar) in only 13 eyes (13%), with no need for injections for at least 12 months. Although effective treatment can prevent blindness in wet AMD patients, the potential for recurrence necessitates continuous follow-up.
Anti-VEGF therapy raises concerns regarding long-term ocular side effects, particularly macular atrophy (MA).
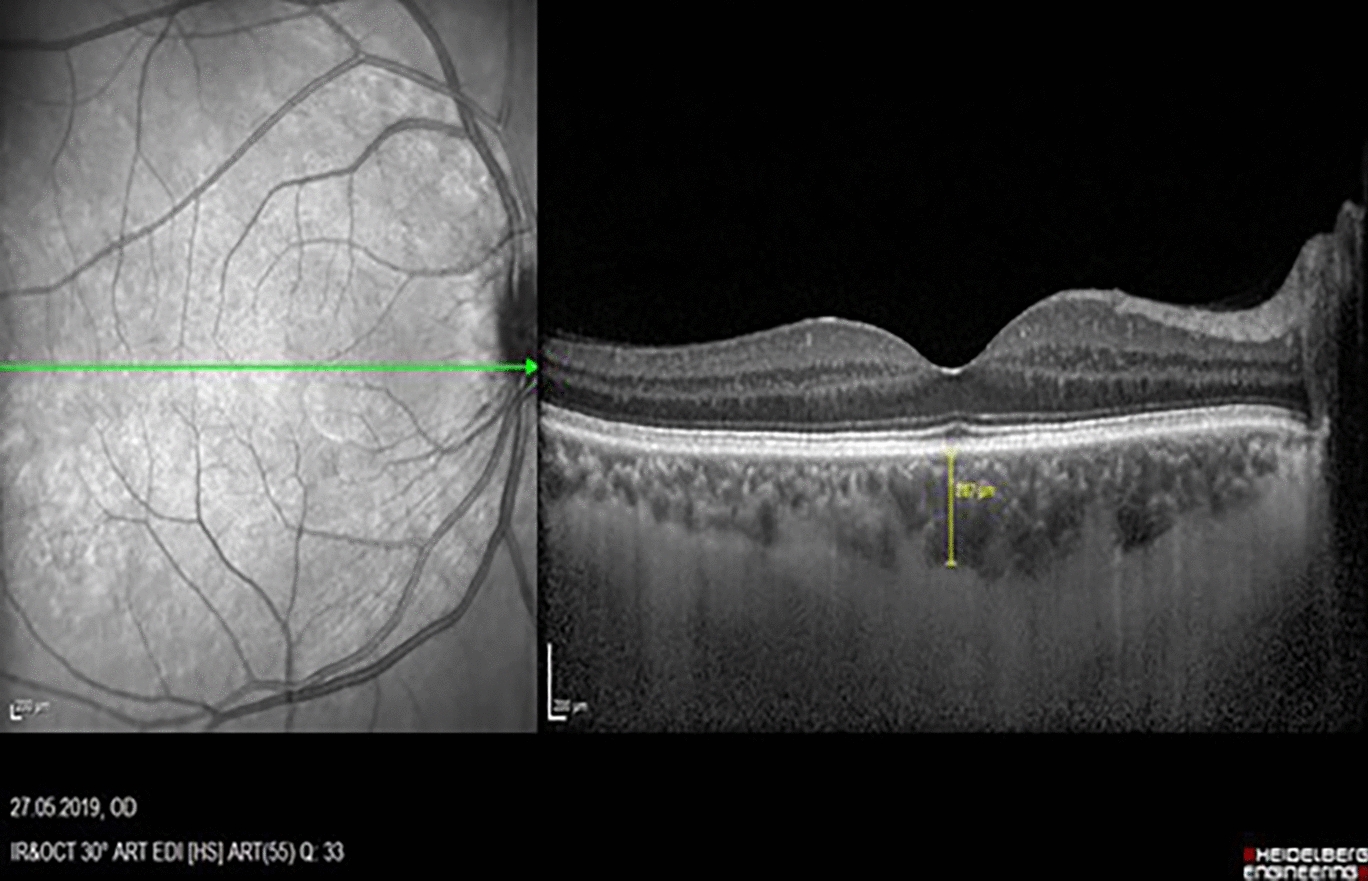
In contrast to geographic atrophy, neovascular atrophy does not exhibit an oval or round shape, and the underlying choroidal vessels may sometimes not visible. Although various imaging modalities have been investigated, a definitive gold standard has yet to be established. Multimodal imaging is widely regarded as the most effective approach [10, 23]. In our study infrared images obtained during OCT imaging were evaluated because of the lack of fundus autofluorescence and colored fundus photography in many cases. Comparing the first and last visit images, progression of macular atrophy was noted in 70 (69%) eyes over an average follow-up period of 10 years, which is consistent with the findings of other studies (Seven up 98%, Munk et al. 74%, Li et al. 53.6%, Tsilimbaris et al. 50.9%) [13, 23,24,25]. MA development is characterized by risk factors including type 3 MNV, choroidal thinning, age, and posterior vitreous detachment [26]. In our study, MA progression was observed more frequently in PDT patients, possibly attributed to additional choroidal thinning. Kawai et al. reported similar results with PDT in their study involving polypoidal choroidal vasculopathy patients [27]. It remains uncertain whether MA development in patients with nAMD is due to disease progression or anti-VEGF treatment. Long-term studies are yet to establish a definitive link between MA and anti-VEGF injections.
The strengths of our study include the substantial sample size (102 eyes) and the extended follow-up period (mean, 116 ± 25 months). Initial examinations included FA for 79 of 82 patients, and both FA and ICG for 41 patients. The study included all patients who received anti-VEGF treatment with follow-ups of at least seven years, irrespective of initial vision, thus avoiding selection bias and reflecting real-life data. A limitation of this study is its retrospective design, a common characteristic of long-term studies, as well as the absence of multimodal imaging for the evaluation of macular atrophy.
In conclusion, for patients with nAMD, visual acuity can be significantly preserved long-term with regular follow-up and consistent intravitreal anti-VEGF treatment.



Comments (0)