
Remember me
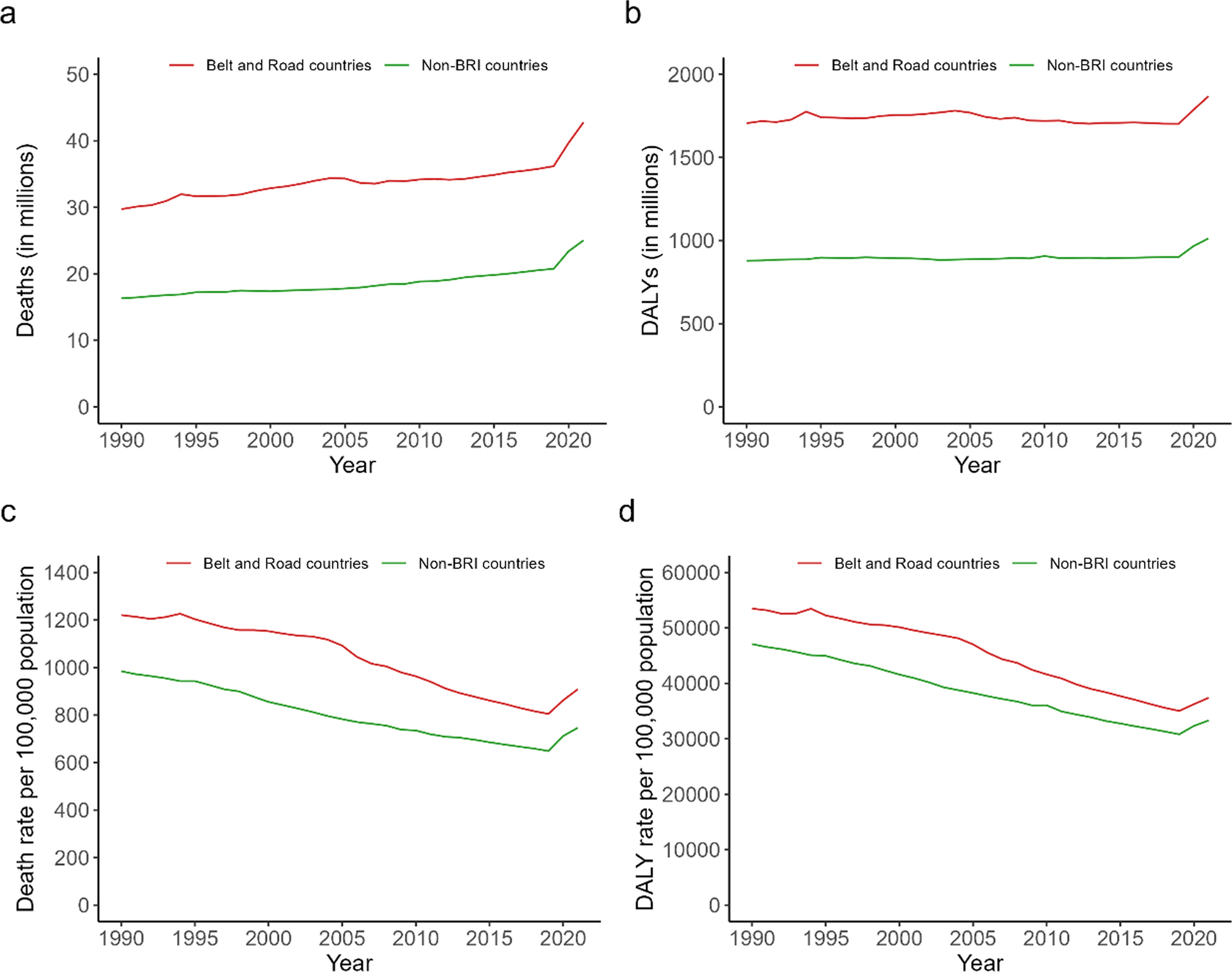

Between 1990 and 2021, the number of deaths and DALYs in the BRI countries accounted for 62.9–66.0% and 64.8–66.8% of global deaths and DALYs, respectively (Online Appendix Table 2). Both the number and rate of deaths and of DALYs were higher in BRI countries than in non-BRI countries during the study time period (Fig. 1a-d). The number of deaths and DALYs increased by 43.9% and 9.5% for BRI countries between 1990 and 2021, respectively, percentages that were similar to 53.3% and 15.3% in non-BRI countries (Fig. 1a, b). In contrast, the age-standardized death rate and DALY rate significantly decreased by 1.45% (95% CI − 1.61% to − 1.30%) and by 1.50% (95% CI − 1.62% to − 1.38%) in BRI countries, and significantly dropped by 1.34%, (95% CI − 1.48% to − 1.20%) and 1.41% (95% CI − 1.49% to − 1.33%) in non-BRI countries (Fig. 1c, d).
Fig. 1
Number and age-standardized rate of deaths and DALYs for 149 BRI countries and for non-BRI countries, 1990–2021 (a number of deaths; b number of DALYs; c death rate; d DALY rate). Note DALY: disability-adjusted life year
Deaths and DALYs by country incomeBetween 1990 and 2021, the number of deaths in the BRI countries increased from 29.7 million to 42.8 million (Online Appendix Table 3), and the number of DALYs increased from 1705.6 million to 1867.7 million (Online Appendix Table 4). UMICs and LMICs consistently had the greatest number of deaths and DALYs, while HICs had the smallest numbers, respectively. The largest increases occurred in UMICs (49.10% increase in deaths number), and HICs (13.90% increase in DALYs number) (Fig. 2a, b).
Fig. 2
Number and age-standardized rate of deaths and DALYs for different income countries, 1990–2021 (a number of deaths; b number of DALYs; c death rate; d DALY rate). Note a. DALY, disability-adjusted life year; b. LICs, low-income countries; LMICs, lower middle-income countries; UMICs, upper middle-income countries; HICs, high-income countries
Between 1990 and 2021, the age-standardized death rate in the BRI countries decreased from 1220.8 to 908.6 per 100,000 population (Online Appendix Table 3), and the age-standardized DALY rate decreased from 53,487.4 to 37,407.7 per 100,000 population (Online Appendix Table 4). LICs consistently had the highest age-standardized death and DALY rate, while HICs had the lowest. The greatest EAPC decrease occurred in HICs for age-standardized death rate (− 1.83%, 95% CI − 1.97% to − 1.69%) and in LICs for age-standardized DALY rate (− 2.03%, 95% CI − 2.20% to − 1.86%) (Fig. 2c, d).
Geographic variations in deaths and DALYsAmong the 149 BRI countries, the age-standardized death rate declined between 1990 and 2021 in 134 countries (89.9%), did not change significantly in 11 countries (7.4%; mostly from African countries), and increased in four countries (2.7%; Montenegro, Libya, United Arab Emirates, and Lesotho) (Fig. 3a and Online Appendix Table 5). The fastest declines occurred in Rwanda (− 3.92%, 95% CI − 4.96% to − 2.87%), the Republic of Korea (− 3.29%, 95% CI − 3.41% to − 3.17%) and Maldives (− 3.21%, 95% CI − 3.42% to − 2.99%). The greatest increases occurred in Lesotho (2.08%, 95% CI 1.39% to 2.77%), Libya (0.83%, 95% CI 0.62% to 1.05%), and Montenegro (0.71%, 95% CI 0.39% to 1.03%) (Online Appendix Table 5).
Fig. 3
Number of age-standardized death and DALY rates by geographical region between 1990 and 2021 in 149 BRI countries (a EAPC in death rate; b EAPC in DALY rate; c age-standardized death rate in 2021; d age-standardized DALY rate in 2021). Notes a. The four categories of age-standardized death and DALY rates in the panels c and d were determined based on quintiles; b. BRI: Belt and Road Initiative; c. DALYs: disability-adjusted life year
The change in age-standardized DALY rate between 1990 and 2021 was relatively consistent across geography (Fig. 3b). The largest decreases occurred in Rwanda (-4.30%, 95% CI -5.48% to -3.11%), Ethiopia (-3.34%, 95% CI -3.60% to -3.08%), and Burundi (-3.08%, 95% CI -3.55% to -2.60%). Three countries experienced DALY rate increases: Lesotho (1.62%, 95% CI 0.92% to 2.33%), Libya (0.39%, 95% CI 0.16% to 0.61%), and Dominica (0.20%, 95% CI 0.02% to 0.38%) (Online Appendix Table 6).
In 2021, the age-standardized death rate varied greatly across the 149 BRI countries. Most African countries had extremely high rates (highest in Lesotho, 3,336 per 100,000 population), while some European countries and a few Asian countries had comparatively low rates (lowest in Singapore, 292 per 100,000 population) (Fig. 3c and Online Appendix Table 5). The age-standardized DALY rate across the 149 BRI countries showed similar variations across geography, with the highest rate in Lesotho (117,885 per 100,000 population) and the lowest in Singapore (14,980 per 100,000 population) (Fig. 3d and Online Appendix Table 6).
The five leading causes of age-standardized death rate and DALY rate were generally similar across the 149 BRI countries in both 1990 and 2021 (Online Appendix Table 7, 8). In 2021, stroke was the leading cause of death and the leading cause of DALYs in 148 countries and 113 countries, respectively. Ischemic heart disease, COVID-19, lower respiratory infections, diabetes mellitus, and chronic kidney disease were the leading cause of death in 139, 138, 64, 43, and 37 countries in 2021, respectively. COVID-19, ischemic heart disease, neonatal disorders, diabetes mellitus, lower respiratory infections were the leading cause of death in 133, 109, 91, 56, and 51 countries in 2021, respectively.
Changes in ten health-related SDGs indicatorsThe EAPC for each of the ten health-related SDGs indicators varied largely across the 149 BRI countries between 1990 and 2021 (Fig. 4). Fifteen countries experienced significant increases between 1990 and 2021 in maternal mortality ratio (mostly African and North American countries). Corresponding increases for the other nine health-related SDGs outcomes were: 1 country for under-five mortality rate (Dominica), 3 for neonatal mortality rate (Dominica, Brunei Darussalam and Zimbabwe), 78 for HIV incidence rate (mostly Asian and European countries), 2 for tuberculosis incidence rate (Lesotho and Philippines), 1 for malaria incidence rate (Venezuela), 5 for NTDs prevalence rate (mostly European countries), 7 for NCD mortality rate (mostly African countries), 21 for suicide mortality rate (mostly African countries), and 7 for road traffic mortality rate (mostly African countries). Accordingly, 121, 147, 143, 58, 143, 78, 136, 130, 108, and 130 countries, respectively, witnessed significant decreases in the ten health indicators (Online Appendix Tables 9, 10, 11, 12, 13, 14, 15, 16, 17 and 18).
Fig. 4
The estimated annual percentage change (EAPC) for 10 key health-related SDGs indicators specifying a concrete target in 149 BRI countries from 1990 to 2021. Notes a. Data points denote the BRI countries having the extreme high and low values of EAPC for each key health-related SDGs indicator; b SDGs: Sustainable Development Goals; c BRI: Belt and Road initiative
Target achievement of ten health-related SDGs indicatorsBased on GBD 2021 estimates and our projections, four health-related SDGs indicators were either achieved in 2021 or are projected to reach their target by 2030 in over half the BRI countries—most from UMICs and HICs in Asia and Europe: 98 countries (66%) for under-five mortality rate, 90 countries (61%) for neonatal mortality rate, 82 countries for malaria incidence rate (55%), and 77 countries (52%) for maternal mortality ratio (Fig. 5 and Online Appendix Tables 19, 20, 21, 22, 23, 24, 25, 26, 27 and 28). In contrast, we projected that the 2030 targets will not be reached in over 70% of BRI countries for the remaining six health-related SDGs indicators. Notably, no BRI countries are projected to achieve the SDGs targets for tuberculosis incidence rate or road traffic mortality rate by 2030.
Fig. 5
Number among 149 BRI countries that have achieved the specified targets for the 10 key health-related SDGs in 2021, or are projected to achieve the targets by 2030. Note BRI: Belt and Road initiative
Comments (0)