
Remember me
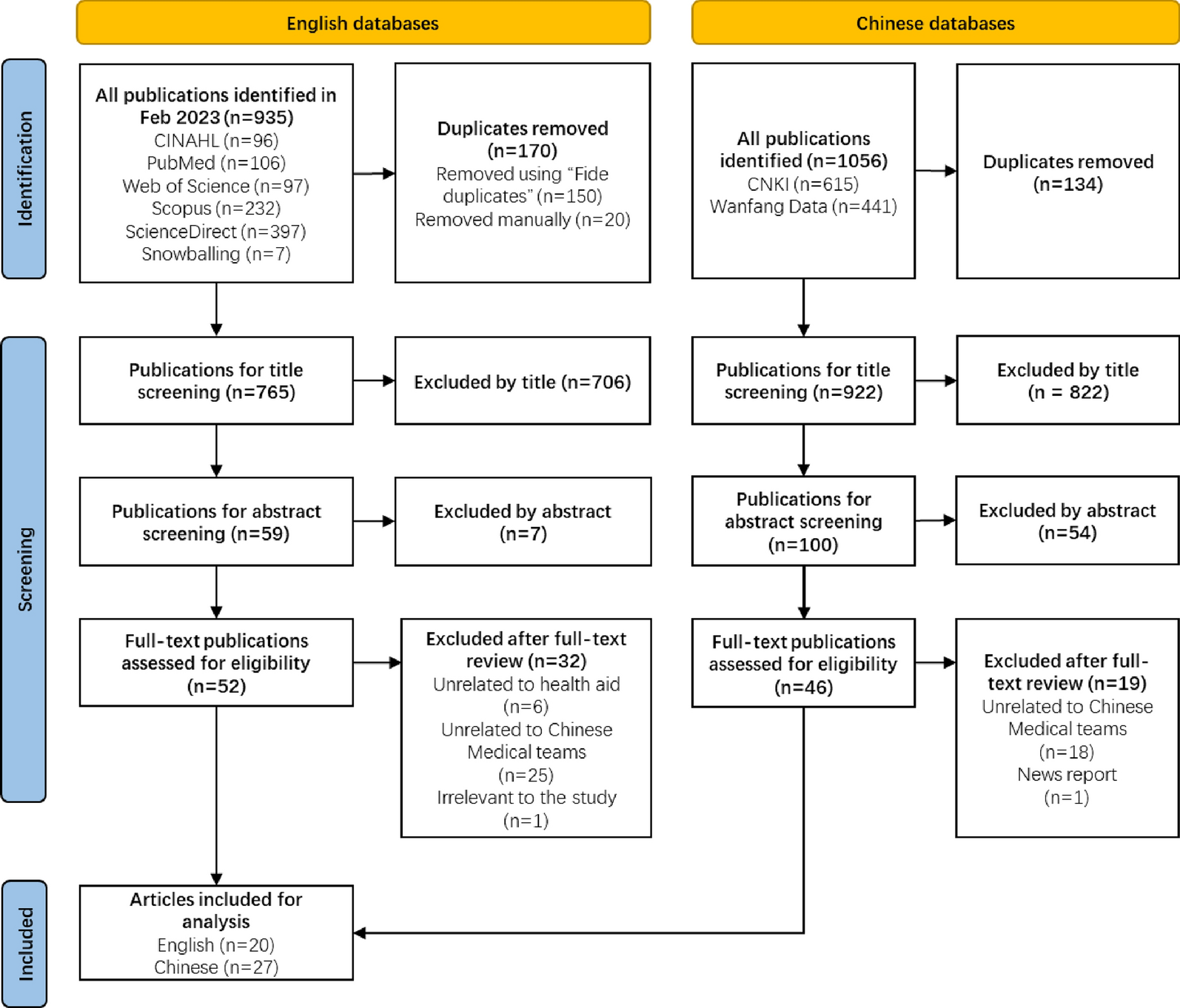
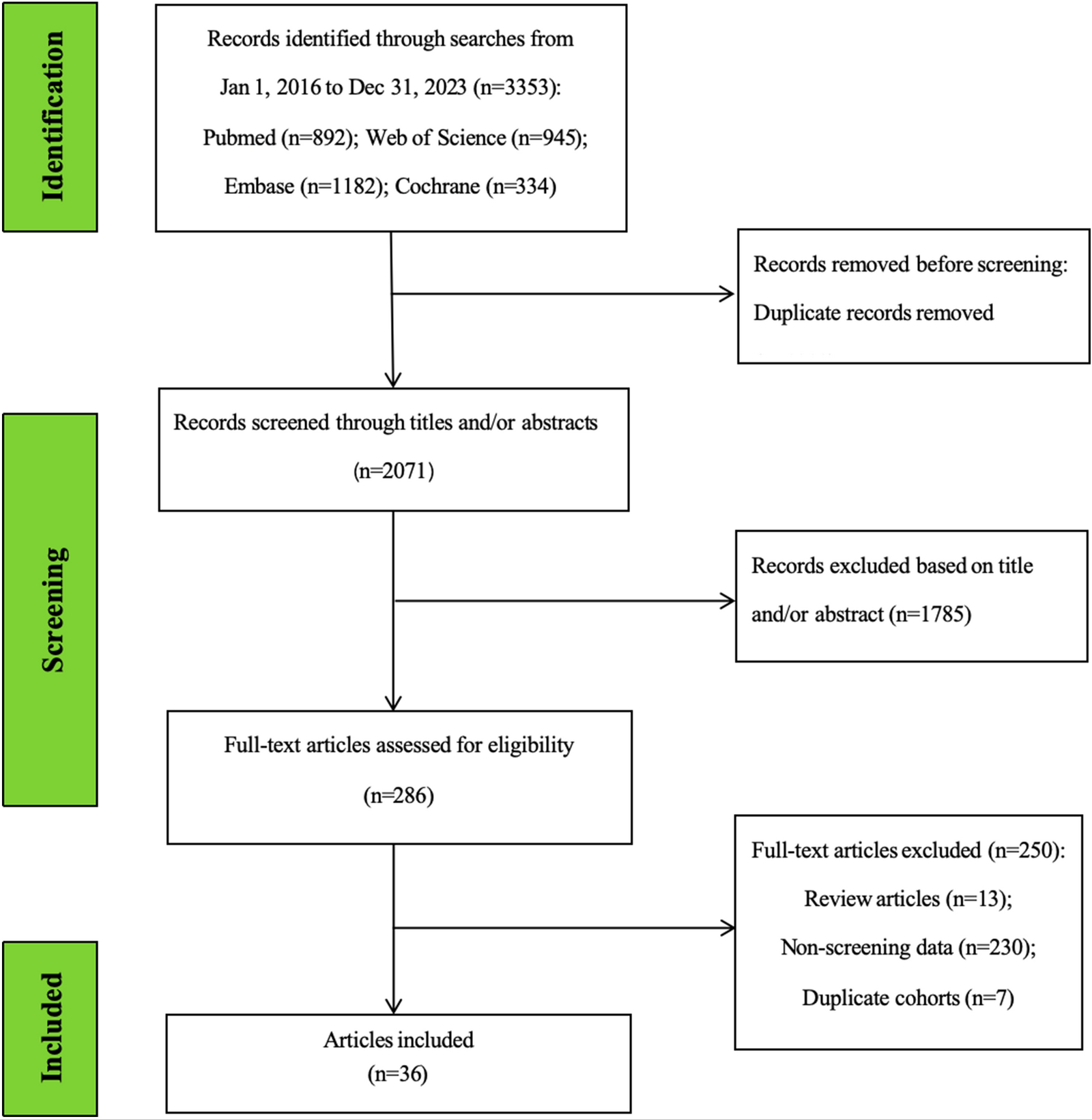

The study selection process is illustrated in the PRISMA-ScR flow diagram in Fig. 1. Initially, a total of 935 English and 1056 Chinese publications were identified. After duplicates were removed, the numbers decreased to 765 and 922, respectively. Subsequent title and abstract screening further narrowed the selection to 52 English and 46 Chinese articles for full-text review. Finally, 32 English articles (6 unrelated to medical aid, 25 unrelated to CMTs, and 1 unrelated to the study) and 19 Chinese articles (18 unrelated to CMTs and 1 news report) were excluded, leaving 20 English and 27 Chinese articles for the final synthesis.
Fig. 1
PRISMA-ScR flow diagram of the study selection process
Characteristics of studies includedTable 1 outlines the characteristics of the 20 English articles included, published between 2009 and 2022. Most of these articles (n = 15) explored the impact of CMTs across multiple African countries. Three articles specifically focused on individual countries. Two articles conducted cross-country comparative analyses. Notably, researchers from China and/or high-income countries (HICs) (U.S., Canada, Sweden) were the first or corresponding authors in 18 of the 20 articles. In comparison, only 2 articles were published collaboratively by researchers from China and other LMICs (Bangladesh and Cameroon). More than half of the articles (n = 11) were published in journals without an impact factor at the time of publication, whereas only 1 review appeared in The Lancet in 2014 (Impact factor: 44.002).
Table 1 Characteristics of the 20 English articles included for evidence synthesis and analysisThe included English articles comprised 10 reviews, 2 viewpoints, and 8 original articles, of which 5 were qualitative and 3 were quantitative. These studies spanned a broad spectrum of health-related issues in African countries, demonstrating the multifaceted contributions of CMTs across the continent. Topics included essential healthcare infrastructure development (n = 12), malaria control (n = 9), the Ebola outbreak (n = 6), health workforce (n = 5), highly infectious diseases including HIV (n = 5), tuberculosis control (n = 3), healthcare service enhancement (n = 3), the COVID-19 pandemic (n = 1), and SARS (n = 1). The interventions undertaken by CMTs, as reported in the articles, included medical team assistance (n = 16), supply of medicines and equipment (n = 11), training of local healthcare professionals (n = 10), provision of financial aid (n = 6), construction of medical facilities (n = 5), health education and promotion (n = 3), and immunisation (n = 1).
The 27 included Chinese articles largely paralleled the English articles in terms of publication period (from 2010 to 2022). A significant number of these articles (n = 18) focused on CMTs’ impact in multiple African countries. Six articles examined individual countries, while three articles conducted comparisons. All but one article, co-authored by researchers from Sudan and China, were published solely by Chinese researchers. About half of the articles (n = 13) were published in Chinese core journals, indicating a high quality of research.
The included Chinese articles comprised 15 reviews, 11 case studies, and 1 ethnographic study. They explored CMTs'contributions to addressing issues including essential healthcare infrastructure development (n = 17), healthcare service enhancement (n = 13), lack of healthcare workers and medicines (n = 13), health workforce development (n = 7), public health (n = 7), control of infectious diseases such as HIV/AIDS, tuberculosis, malaria, and schistosomiasis (n = 9), as well as Ebola (n = 3), COVID-19 (n = 4), and rehabilitation medicine (n = 1). Reported CMT programmes included medical team assistance (n = 20), supply of medicines and equipment (n = 18), training of local healthcare professionals (n = 16), technical cooperation and exchange (n = 16), construction of medical facilities (n = 17), public health assistance (n = 9), Chinese medicine (n = 9), short-term programmes such as the “Brightness Action” (n = 6), health education and promotion (n = 4), and immunisation (n = 1). While only English-language studies are cited in the text, an overview of the 27 Chinese studies and a summary of their key findings are provided in Supplementary Material: Appendix 5 for reference.
Modality of CMT programmesProgramme location. The first CMT was deployed to Algeria in 1963, marking the beginning of CMT medical aid in Africa [11, 12, 14, 15, 23,24,25,26,27,28,29,30,31,32]. This dispatch was characterised by a “no strings attached” approach, denoting the provision of aid without any political, economic, or ideological conditions [15, 32]. By the end of 2013, 1171 CMTs had operated in 113 medical centres across 49 recipient countries, with 42 of these countries located in Africa [24, 33,34,35,36,37,38]. A significant portion of the teams served in rural areas [12, 14, 15, 31] where local medical coverage was insufficient [12]. Meanwhile, the establishment of 30 anti-malaria centres by 2013 exemplified the targeted efforts of CMTs to combat specific health challenges [28].
Programme duration. The duration of CMT programmes has ranged from a few months to over two years [14, 24, 26, 27, 30, 35, 36]. Short-term missions addressed immediate healthcare needs, such as during the 2014–2015 Ebola outbreak when CMTs provided treatment, infection control, and medical supplies, significantly mitigating the virus’s impact in African communities [35, 36]. Conversely, the long-term deployments aimed to foster sustainable healthcare improvements [24]. These missions, which included training local health professionals and establishing essential healthcare infrastructure such as hospitals, clinics, and malaria control centres [27], were designed to lay a lasting foundation for the ongoing enhancement of healthcare systems in recipient countries [24, 26, 27].
Collaborative initiatives. CMTs have collaborated with multiple local healthcare teams in Africa [12, 14, 23,24,25, 27, 28, 30,31,32,33, 35,36,37,38], which comprised doctors, nurses, project directors, health facility administrators, Ministry of Health officials [14, 25, 32], and representatives from non-governmental organisations [33]. The multisectoral partnerships delivered a broad range of services, from primary care to specialised treatments [14, 24, 33]. A large focus of these initiatives was on controlling and eradicating malaria [23, 24, 27, 28, 30, 31, 33, 37, 38], as well as managing other infectious diseases like measles, filariasis, schistosomiasis, HIV/AIDS, and tuberculosis [12, 27, 30, 31, 33], alongside responses to pandemics such as SARS, Ebola, and COVID-19 [12, 25, 30, 31, 35, 36]. These efforts included comprehensive strategies like vaccination campaigns and mass drug administration [12]. Meanwhile, CMTs actively tackled non-communicable diseases through short-term programmes [12, 24, 25, 33]. For instance, under the “Heart-to-Heart” programme, 170 heart surgeries were carried out in Ghana and Tanzania, while the “Brightness Action” programme facilitated 9,752 cataract surgeries in 25 countries, including Botswana, Eritrea, and Morocco [12]. Furthermore, to enhance healthcare delivery, Chinese partnerships have built hospitals, expanded local pharmaceutical production, and established over 10 clinics that integrate traditional Chinese and African medicines in remote African areas [24, 28, 31].
Resources and expertise. The composition of CMTs included seasoned professionals such as doctors and nurses specialised in infectious diseases, surgery, gynaecology, ophthalmology, and obstetrics [12, 14, 15, 23, 24, 26,27,28,29,30,31,32,33, 35,36,37], as well as public health experts [12, 35]. The teams also included translators [24, 26] and administrative support staff [30], who facilitated the smooth execution of initiatives. Provincial governments in China, such as Ningxia, Guangxi, Tianjin, and Shanghai, were responsible for deploying medical teams to specific African countries like Benin, Comoros, Gabon, and Cameroon [15, 23, 27, 30]. These teams were strategically stationed in local hospitals and clinics [37], allowing the direct allocation of resources, including medical supplies and training courses tailored to the specific needs of recipient countries [14, 24, 29, 31, 33, 36].
Effectiveness of CMT programmesMeeting local healthcare needs. Local clinics and hospitals that benefited from CMT programmes reported a reduction in patient load related to common illnesses, evidencing the effectiveness of these initiatives [12, 28, 31, 35, 38]. Campaigns like “Brightness Action” and “Heart-to-Heart” were highly praised for significantly improving specific health outcomes, particularly in rural areas [12]. Moreover, the literature demonstrates the effectiveness of CMTs in controlling infectious diseases. For example, a malaria control initiative in the Plateaux Region of Togo in 2017 reduced the infection rate from 79 to 37% [
Comments (0)