Dementia is one of the leading causes of neurological burden worldwide. Compared to the previous GBD 2019 publication, our study indicates that, despite notable achievements over the past 32 years, health disparities in dementia burden— particularly in terms of dementia mortality—appear to be widening globally [15, 16]. For instance, the global ASMR shifted from an increasing trend between 1990 and 2019 to a decreasing trend from 1990 to 2021 [16]. However, the ASMR only decreased in high SDI region from 1990 to 2021, suggesting a growing geographical gap in the progress of dementia control initiatives [16]. Our analysis of GBD dementia incidence and prevalence suggests that many countries have experienced a decline in dementia incidence and prevalence. However, countries in East Asia and High-income Asia Pacific, particularly China, have shown little or no progress. Dementia is emerging as one of the leading causes of mortality globally, and mortality due to dementia is expected to increase in the future due to corresponding increases in population growth and aging [16]. Our analysis of GBD mortality rate and DALYs rate suggests that only high SDI region have experienced a decline in GBD mortality rate and DALYs rate. However, economically disadvantaged countries in South Asia, Central Sub-Saharan Africa, and Southern Sub-Saharan Africa have shown no progress. More than one third of countries and territories experienced an increasing trend in mortality rate, particularly in India. The trend of dementia incidence was correlated with supply of HRH (personal care workers, psychologists, physicians). The trend of dementia mortality was commensurate with country-level socioeconomic status and supply of HRH (psychologists, physicians). We also found that the early-onset dementia incidence and mortality are increasing significantly in North Africa and Middle East, and Central Sub-Saharan Africa, respectively, especially among females. This highlights the importance of healthcare systems for dementia that cover the early midlife span.
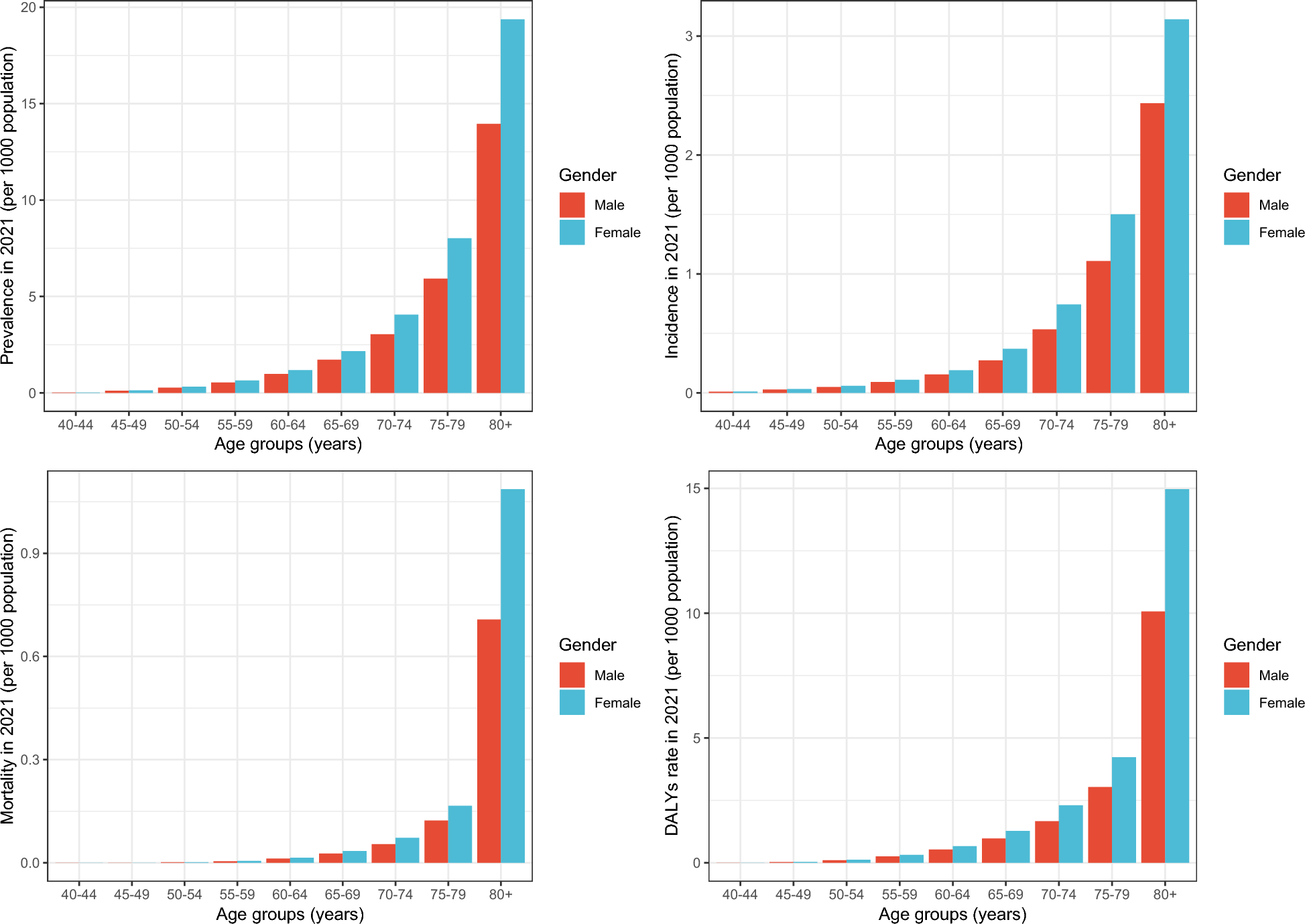
This study used data from the 2021 GBD study to systematically evaluate global trends and regional differences in dementia burden. Although the prevalence and incidence remained stable or slightly decreased worldwide, the absolute number of prevalent cases and incident cases increased by more than 150% from 1990 to 2021. The substantial number of prevalent cases and incident cases continues to pose a significant challenge [17]. In comparison to other regions, East Asia and High-income Asia Pacific exhibited a notable upward trend in both prevalence and incidence. The concurrent marked regional disparities in the escalation of these rates suggest a potential imbalance in preventive initiatives against dementia over the past several decades. The Global dementia action plan address this issue by establishing a global target for 75% of WHO Member States to have developed or updated a national policy, strategy, plan, or framework for dementia—either as a stand-alone initiative or integrated into other policies—by 2025 [4, 17]. However, only 50 countries (26% of Member States) met this target in 2021 [4, 17]. Meanwhile, the distribution of national dementia plans is largely uneven across WHO regions, with half of the policies (n = 26) originating from the European Region [4]. Despite a significant number of countries having plans or guidelines for reducing dementia risk, approximately 78% of these countries are high-income countries [4]. The number of countries and territories experiencing increasing prevalence and incidence of dementia has been nearly a quarter of all countries worldwide from 1990 to 2021, which represents a decline compared to the period from 1990 to 2019, underscoring the importance of national dementia plans [18]. Currently, it is imperative that prevention programs be prioritized in the East Asia and the High-income Asia Pacific regions, alongside the ongoing implementation of existing initiatives in other areas. Additionally, we found that the global prevalence, incidence and mortality were higher among females than males. It is important to note that the factors contributing to the observed demographic variations in dementia burden between females and males are complex, involving various biological, social, and environmental influences [19]. Among these, the longer life expectancy of females compared to males is a common potential factor, indicating that females are more likely to reach the age ranges where the risk of dementia is elevated [20]. Furthermore, declining estrogen levels, related oophorectomy, and historically lower education levels among females may also be contribute to this disparity [19]. In any case, the current gender differences in dementia burden suggest that further exploration of the mechanisms underlying these differences is necessary, along with the implementation of measures to mitigate the higher burden experienced by females.
The escalating prevalence and incidence of dementia are placing a significant burden on the public and healthcare systems in China. One meta-analysis showed that the prevalence and incidence of dementia increased with age and over time in China from 2010 to 2020 [21]. Contributing factors may include the growing aging population, changes in lifestyle habits, and a high burden of vascular-metabolic multimorbidity may all be causes [3, 22]. Additionally, a decline in cultural and social engagement may further exacerbate the progression of dementia [23]. In China, despite improved access to health services, inadequate management of dementia remains common, particularly in rural areas [24]. As the primary health care institutions may be more concerned about diabetes, hypertension, and chronic obstructive pulmonary disease, etc. in the past years, the existing three—tier long-term care system is still insufficient to meet the needs of individuals with dementia [25]. China still needs to prioritize future improvement in primary health care institutions, focusing more on prevention of dementia, within the context of the highest ASPR and ASIR in 2021 and the highest increasing trend of these two indicators from 1990 to 2021. Establishing a national surveillance system to monitor the incidence, prevalence, and the risk and protective factors associated with dementia is essential. Our findings indicate that the trend of dementia incidence is correlated with the availability of HRH (personal care workers, psychologists, physicians) from 2019 to 2021. Within the framework of the Chinese healthcare system, community multidisciplinary teams and care home intervention teams in primary and secondary hospitals could be instrumental in achieving the goal of dementia prevention [25,26,27]. Additionally, multi-center national clinical trial centers should be established, particularly for traditional Chinese medicines, which, despite its popularity among many dementia patients, lacks substantial evidence supporting efficacy [24].
Progress in deceasing dementia-related deaths appears minimal. The global mortality rate has decreased by only 0.02%, yet more than one-third of countries have experienced an upward trend in mortality rates. Specifically, the mortality rate has significantly increased in low SDI region and low-middle SDI region. The trend of dementia mortality are commensurate with country-level socioeconomic status, indicating the need for enhanced support, particularly in LMICs. The Global status report on the public health response to dementia shows that community-based services for dementia are more prevalent in high-income countries compared to LMICs [4]. Access to medication for dementia, hygiene products, assistive technologies, and household modifications is more readily available in high-income countries due to higher levels of reimbursement compared to lower-income countries [4]. Recently, there has been a consolidated trend toward multi-component interventions for dementia progression, particularly evident in the World-Wide Finnish Geriatric Intervention Study (WW-FINGERS) to prevent cognitive impairment and disability [5]. The FINGER study highlighted the importance of addressing multiple dementia risk factors as a strategy to protect brain health, promote overall health and reduce the risk of developing new chronic diseases [5, 28, 29]. However, multidomain intervention trials in LMICs are currently lacking [5, 29].
We also found that the early-onset dementia incidence and mortality are increasing most significantly in North Africa and Middle East, and in Central Sub-Saharan Africa, respectively. This suggests that the gaps and barriers hindering effective action may be widening throughout the midlife span. In comparison to the limited number of low-income or lower-middle income countries with a national dementia plan, the number of high-income countries with such plans is considerably higher. Nearly one third of upper-middle-income countries and half of high-income countries have reported national or subnational dementia research plans [4]. Given the complexity of dementia, it cannot be effectively addressed in isolation. The underrepresentation of low-income or lower-middle income countries, due to limited funding and inadequate research capacity, along with the exclusion of individuals with dementia and their caregivers from research development impedes inclusivity [4]. We found that the ASMR increased the most in low SDI region, followed by low-middle SDI region. Additionally, the highest ASMR was observed in the DRC in 2021. It is possible that the lag in relevant research in lower-income countries has made it challenging to address the dementia burden, particularly in terms of reducing mortality. Effectively decreasing the risk of deaths attributed to dementia relies on robust clinical medical evidence and sound policy management. As proposed by the WHO, it is urgent to enhance research collaboration and establish a global coordination mechanism to support worldwide innovation in the approach to dementia [4].
Our study provides an in-depth analysis of dementia trends using the latest GBD data to understand disparities in the prevention and management of dementia within the context of an aging population. A notable limitation of this analysis is that the accuracy and robustness of GBD estimates largely depend on the quality and quantity of data used in the modeling [30]. In countries where national systematic surveillance and population-based studies are lacking or insufficient, the estimates may be subject to bias.


Comments (0)