
Remember me



From January 1st, 2012, through December 31, 2021, a total of 1355 patients were screened. Two hundred and twenty-nine of them presented a suspected pleural infection and were included, including 91 patients treated by RTT and 138 by CTD, respectively. Characteristics of all patients included are summarized in Supplementary Table 1.
The median age was 63 years old (IQR [50–75]) and most patients were men (n = 166/229, 72%). Alcoholism and swallowing disorders were more frequent in the RTT group. However, there was no significant difference regarding the other comorbidities. Seventy-five percent of pleural infections were community-acquired (n = 171/229). In the RTT group, patients had more symptoms at initial presentation such as fever, cough, chest pain and dyspnea. There were 60% of empyema in the RTT group compared to 64% in the CTD group. The use of CT scan (n = 208/229, 91%) and thoracic ultrasound (n = 194/229, 85%) revealed presence of loculations in 66% of cases (n = 150/229). Pleural fluid culture was positive in 58% of patients, most commonly for Streptococci of anginosus group (n = 60/229, 26%) or anaerobes (n = 47/229, 21%). In the RTT group, Streptococcus pneumoniae was more frequently identified than in the CT group (22% vs 4%).
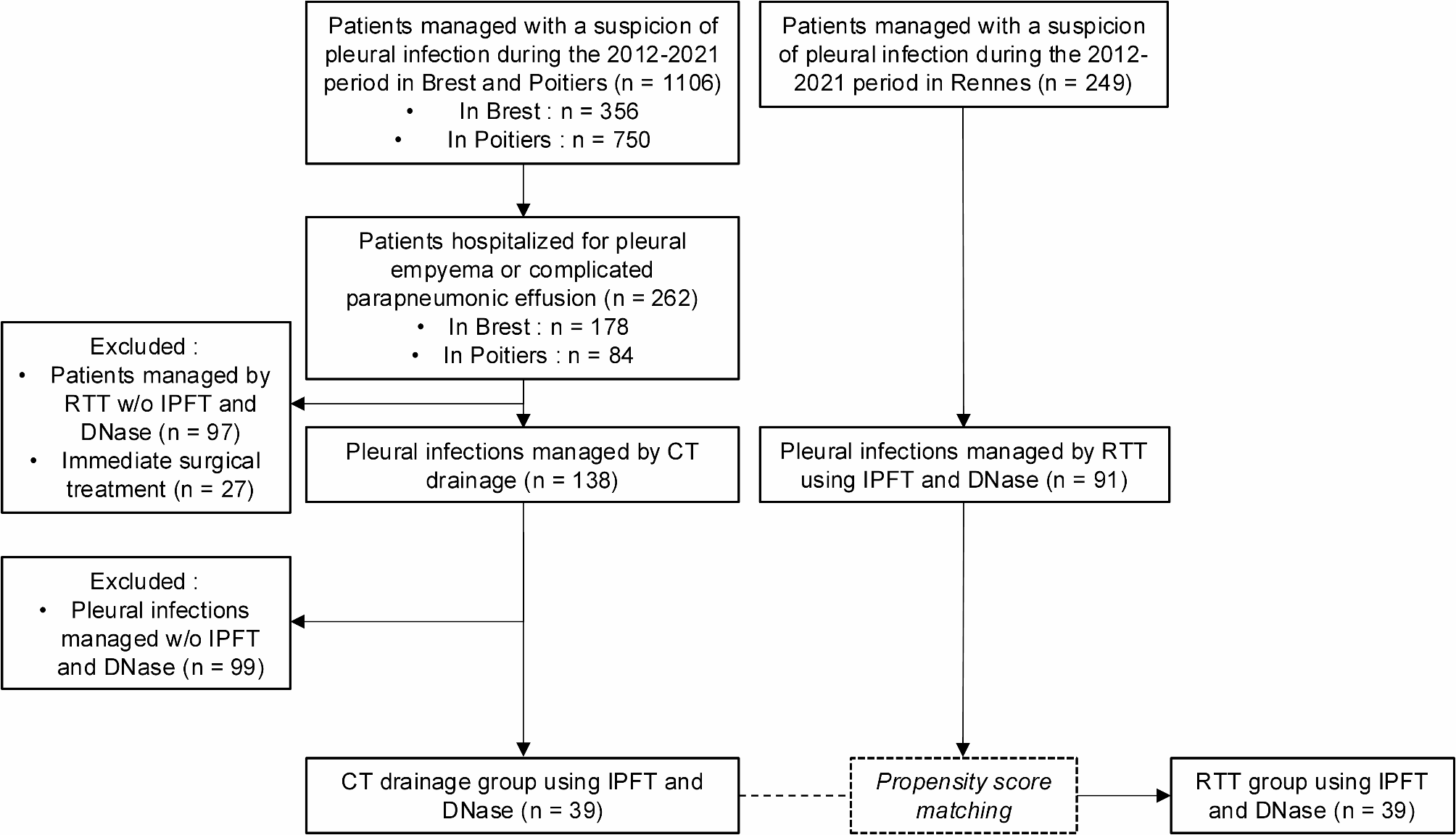
Propensity-score matched populationOne hundred and thirty patients fulfilled criteria of pleural infection managed by pleural drainage and receiving IPFT plus intrapleural DNase in the three participating centers. After matching, 78 patients were included in the final analysis, divided in two groups of 39 patients each (Fig. 1). One group received IPFT plus DNase through CT (CTD group), and the other group was managed using RTT with at least one instillation of urokinase plus DNase (RTT group).
Fig. 1
Flowchart of the study
CT= Chest Tube; IPFT = Intrapleural Fibrinolytic Therapy; RTT = Repeated Therapeutic Thoracocentesis
Characteristics of each group are described in Table 1. In the population, 71% were men (n = 55/78) and the median age was 60 years (IQR [51–71]). Most of pleural infections were community-acquired (n = 55/78, 71%). The two groups were comparable for the following variables: age, sex-ratio, medical history of smoking, alcoholism, previous pleural infection, immunodepression, diabetes mellitus, malignancy and use of immunosuppressive treatments. Swallowing disorders were more frequent in the RTT group (18% vs 5%).
Table 1 Baseline characteristics of the study population with use of intrapleural fibrinolytic and DNaseIn the RTT group, patients had more symptoms at initial presentation, especially more fever (77% vs 59%), cough (74% vs 33%), sputum (41% vs 21%) and dyspnea (85% vs 72%). Signs of respiratory distress were numerically higher at the admission in the RTT group (33% vs 15%).
Biological data and imaging features were similar in both groups. Hilar or suprahilar effusion was reported in 73% of patient (n = 57/78). Intrapleural loculations were present in 73% of cases (n = 57/78). Pleural fluid culture was positive in half of cases (n = 40/78, 51%). The anginosus group streptococci were the most common bacteria (n = 20/78, 26%), followed by strict anaerobes (n = 11/78, 14%) and Streptococcus pneumoniae (n = 8/78, 10%).
In the RTT group, a median of 4 thoracocenteses [3–6] were performed, with a median interval of 6 days between the first and last thoracocentesis (Table 2). In the CTD group, median drainage duration was 9 days [6.5–13]. The total number of administrations of IPFT plus DNase in the two groups were similar (n = 3, [2–5]). Urokinase was the only fibrinolytic agent used in the RTT group, whereas alteplase was mostly used in the CTD group (alteplase use = 89%, urokinase use = 11%). Saline lavages occurred only in the CTD group (n = 35/39, 90%). The most common complication was chest pain which required the use of morphine in 42% of cases. Iatrogenic pneumothorax (n = 6/78, 8%), iatrogenic hemothorax (n = 6/78, 8%) and thromboembolic disease (n = 5/78, 6%) were less frequent.
Table 2 Clinical management in the matched populationMedian duration of intravenous antibiotics (13 days, [7–24]) and median total duration of antibiotic therapy (42 days, [28–43]) were comparable in the two groups. Amoxicillin/clavulanic acid (n = 36/78, 46%) and ceftriaxone/metronidazole (n = 18/78, 23%) were the two most common empirical regimen used. Then, half of patients pursued orally amoxicillin/clavulanic acid (n = 38, 49%) or amoxicillin only (n = 18, 23%). Most of patients received chest physiotherapy (n = 69, 88%) during hospitalization.
OutcomesAfter propensity-score matching (Table 3), there was no significant difference in in-hospital (OR = 0.95, 95%CI [0.84–1.07]) or one-year mortality (OR = 0.79, 95%CI [0.85–1.24]) between the two groups. Eight percent of patients died during hospitalization and 17 patients died within the first year (22%). Drainage failure occurred in 26% of patients and secondary surgical referral was needed for 12% of them, but no difference was found between RTT and CTD groups (OR = 1.03, 95%CI [0.83–1.27] and OR = 0.97, 95%CI [0.84–1.13] respectively). More precisely, causes of RTT failures were as follows: three patients were referred to surgery, one patient had only blank thoracenteses (< 50 mL retrieved, but IPFT plus DNase could have been administered), one patient was transferred to ICU due to increased oxygen flow (but no need for CTD insertion), one patient died of sepsis, and one patient required chest tube drain insertion after RTT failure. Patients in RTT group had a reduced length of drainage (6 days [4.3–8] vs 9 [6.5–13], OR = 1.41, 95%CI [1.05–1.89]) and a reduced length of hospital stay (15 days [11.5–21.5] vs 21 [14–30.5], OR = 1.41, 95%CI [1.05–1.89]). No significant difference was found for rehospitalization for relapse.
Table 3 Outcome comparison between CTD and RTT groups after overlap propensity-score matched analysisNo substantial difference was found in drainage complications rates (OR = 1.17, 95%CI [0.94–1.45]) between RTT and CTD procedures. Just under half of patients (n = 33/78, 42%) used morphine due to chest pain, which constituted the primary complication associated with pleural drainage. Iatrogenic pneumothorax and hemothorax were low in both groups but more frequent in the CTD group than in the RTT group, with rates of 10% (vs 5%) and 13% (vs 3%).
Comments (0)