This first real-world study aimed to assess the effectiveness of novel oral antiviral agents in managing COVID-19 among high-risk patients during the Omicron JN.1 subvariant wave. Through PSM and analysis of data from the TriNetX platform, we identified significant reductions in short-term adverse outcomes among patients receiving oral antiviral treatment compared to those not receiving antiviral agents. Specifically, oral antiviral agents were associated with a significant 23% reduction in the risk of all-cause ED visits, hospitalization, or mortality. Furthermore, they were associated with a 22% reduction in the risk of ED visits, a 14% reduction in the risk of hospitalization, and an impressive 83% reduction in the risk of death. These findings remained consistent across most subgroup analyses, irrespective of age, sex, underlying disease, the episode of infection, and the type of antiviral agents used. Such consistency underscores the robustness of the observed benefits of oral antiviral therapy across diverse patient populations. These results align with previous studies demonstrating the efficacy of oral antiviral agents, such as NMV-r or MOV, in reducing the severity and duration of illness in COVID-19 patients infected with other SARS-CoV-2 variants prior to the Omicron JN.1 subvariant wave [29,30,31,32,33,34,35,36,37,38,39]. The study's findings add to the growing body of evidence supporting the potential benefits of oral antiviral agents in treating COVID-19. They underscore the importance of early intervention with oral antiviral therapy, particularly in high-risk patient populations. By reducing the risk of severe outcomes, including hospitalization and death, oral antiviral agents offer a promising therapeutic option for managing COVID-19 and mitigating its impact on healthcare systems and public health.
Despite consistent benefits observed across almost all subgroup analyses, indicating the potential effectiveness of oral antiviral agents across diverse patient populations, there was a notable difference in the subgroup analysis of individuals with and without booster vaccination. While significant benefits of oral antiviral treatment were evident in individuals without booster vaccination, there was a lack of significant benefit observed in those who had received booster vaccination. This finding aligns with previous research suggesting that effective vaccination can prevent the progression of COVID-19 and may attenuate the effects of antiviral treatment [39, 40]. However, it is worth noting that only a small proportion of patients in our study population had received booster vaccination, constituting less than 2% of the total before PSM. Consequently, oral antiviral agents remain an effective therapeutic option for the vast majority of patients included in this real-world study. Nonetheless, further investigation is warranted to elucidate the underlying mechanisms behind this observation and to comprehensively evaluate the impact of booster vaccination on the outcomes of antiviral treatment. it is crucial to recognize that only a small fraction of patients in our study population had received booster vaccination, comprising less than 2% of the total before PSM. As a result, oral antiviral agents retain their status as an effective therapeutic choice for the overwhelming majority of patients enrolled in this real-world study. However, there is a pressing need for further investigation to uncover the underlying mechanisms driving this observation and to conduct a comprehensive assessment of the impact of booster vaccination on the outcomes of antiviral treatment. In the meanwhile, healthcare authorities should actively seek to understand the reasons behind vaccine hesitancy and fatigue and develop effective strategies to enhance the uptake of booster vaccines. By promoting vaccination uptake and ensuring widespread coverage of booster doses, healthcare systems can strengthen their response to the ongoing COVID-19 pandemic and reduce the burden of disease on individuals and communities.
The findings of this real-world study also revealed that less than one-third of individuals with an elevated risk for disease progression received antiviral agents, suggesting that a substantial proportion of patients who could potentially benefit from antiviral treatment did not receive these effective interventions. Several factors may contribute to the underutilization of antiviral therapy in this population. First, concerns about the risk of drug-related adverse effects may deter healthcare providers from prescribing antiviral agents, particularly in patients with underlying comorbidities. Second, healthcare providers may be concerned about potential drug-drug interactions between antiviral agents and other medications commonly used to manage comorbidities in high-risk patients. Lastly, poor accessibility to antiviral medications may present a barrier to treatment initiation for high-risk COVID-19 patients. However, addressing these barriers to antiviral therapy is paramount to ensure equitable access to effective treatments for high-risk COVID-19 patients. Healthcare systems must prioritize efforts to educate providers about the benefits and safety profile of antiviral agents, enhance surveillance and management of potential drug interactions, and improve the availability and accessibility of antiviral medications. Additionally, strategies to mitigate barriers related to cost, distribution, and healthcare access are essential to ensure that all eligible patients have the opportunity to receive timely and appropriate antiviral treatment. By addressing these challenges, healthcare providers can optimize the management of high-risk COVID-19 patients and reduce the burden of severe illness and mortality.
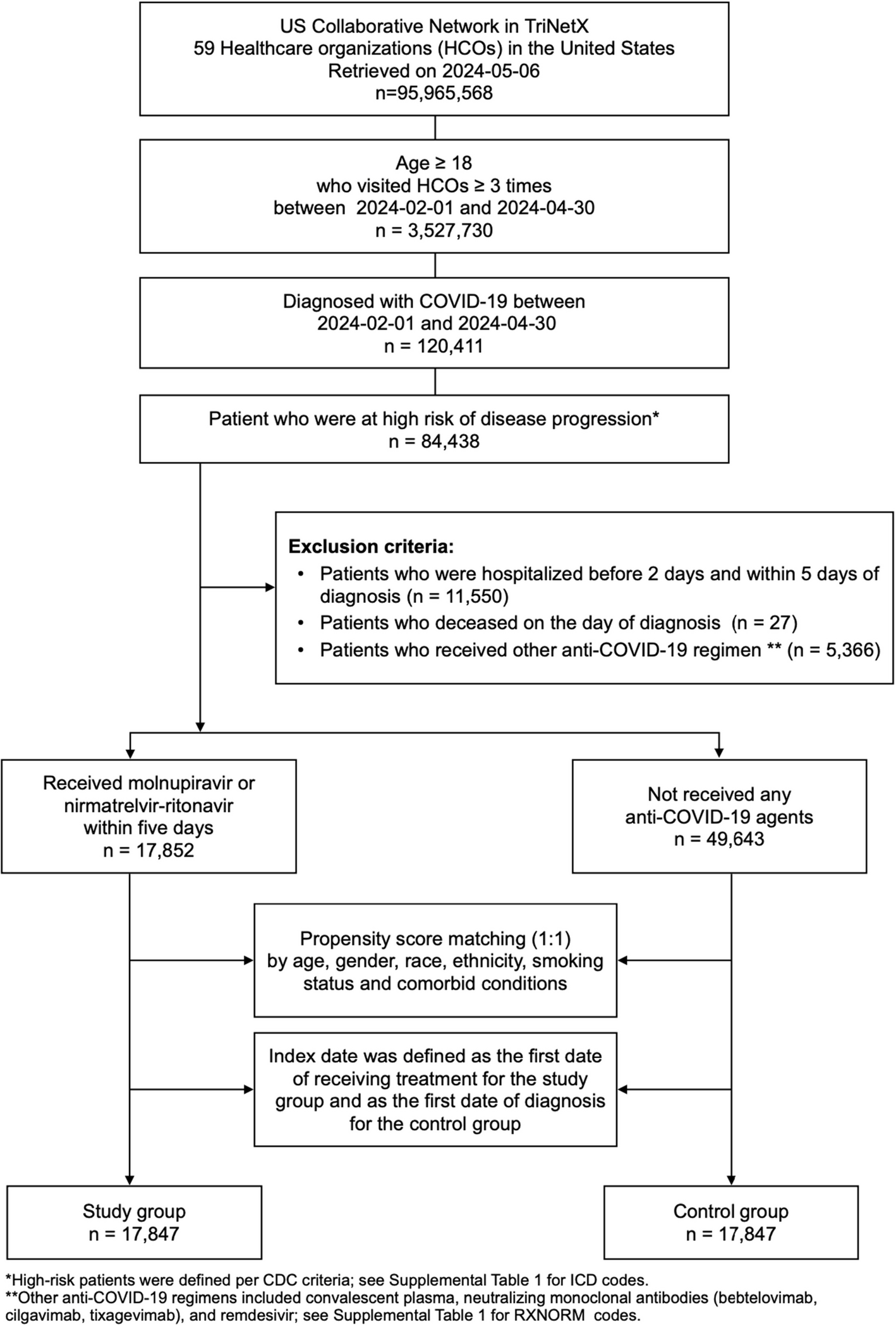
This study had several strengths. By utilizing epidemiological data from the United States CDC and the US Collaborative network through the TriNetX platform, we were able to identify the cohort particularly affected by the Omicron JN.1 epidemic. Leveraging a large, multi-institutional database allowed us to capture a substantial and diverse patient population involved in the Omicron JN.1 wave. The inclusion of comprehensive patient data, such as demographic characteristics, comorbidities, and treatment information, enabled detailed subgroup analyses and enhanced the generalizability of our findings. PSM was used to minimize confounding factors, aligning our study with Target Trial Emulation principles. Given this robust design, we believe that our analysis of the Omicron JN.1 wave in the US could serve as a valuable resource for the global response to the Omicron JN.1 wave.
However, several limitations should be acknowledged. First, as with any retrospective study, selection bias and unmeasured confounding cannot be entirely ruled out. While PSM was applied to balance baseline characteristics, residual confounding may persist, particularly due to the lack of detailed severity metrics such as the WHO severity score and Charlson Comorbidity Index. However, to minimize this issue, we included only outpatient antivirals per IDSA guidelines for mild-to-moderate disease and excluded patients requiring hospital-level care. Second, requiring at least three medical visits within three months may have favored patients with higher health-seeking behavior or greater disease severity, potentially limiting generalizability. However, this criterion was necessary to ensure regular follow-up, minimize loss to follow-up, and maintain comprehensive case capture for outcome analysis. Despite this, some patients may have sought care outside the TriNetX network, leading to potential underestimation of certain events. This is an inherent limitation of database studies. Third, reliance on electronic health record data may introduce errors or inconsistencies in coding and documentation, affecting the accuracy of outcome ascertainment. For example, patients in the control group may have received antiviral treatment outside the network, which was not captured in our dataset, potentially leading to misclassification bias. The TriNetX database also does not provide disease-specific or COVID-19-related emergency department visits, hospitalizations, or mortality, which may result in overestimation or underestimation of these outcomes. Further real-world studies specifically evaluating COVID-19-related emergency visits, hospitalizations, and mortality are needed. Additionally, the definition of the index date may introduce potential immortal time bias, as patients in the study group must survive until antiviral initiation. However, since antiviral treatment was required to be initiated within 5 days of symptom onset, the window for immortal time was minimal. To further address this concern, we conducted a sensitivity analysis excluding patients who died within 5 days of COVID-19 diagnosis, and the results aligned with our study outcomes (Supplemental Table 5). Furthermore, the small sample size of the booster-vaccinated subgroup limited statistical power, making it difficult to detect a significant effect. The observed lack of benefit in this group may be due to low event rates rather than an actual absence of efficacy. Besides, the observational nature of the study precludes causal inference, and further randomized controlled trials are needed to confirm the efficacy of oral antiviral agents in managing COVID-19. Lastly, due to epidemiological constraints, this study focused exclusively on the Omicron JN.1 wave in the US, where government policies, public health strategies, and patient characteristics might differ from those elsewhere in the world. Specifically, only FDA-approved oral antivirals were considered, excluding novel agents such as ensitrelvir and other emerging treatments approved elsewhere but not yet in the U.S. This may limit the generalizability of our findings to settings where these newer treatments are available.
In conclusion, our study demonstrated the effectiveness of novel oral antiviral agents in mitigating the progression of COVID-19 among high-risk patients during the Omicron JN.1 subvariant wave. This real-world study provides updated and robust evidence supporting the effectiveness of oral antiviral agents in managing COVID-19 among high-risk patients during the Omicron JN.1 subvariant wave. The significant reductions in adverse outcomes observed underscore the importance of early intervention with oral antiviral therapy, particularly in vulnerable populations. However, the lack of significant benefit observed in individuals with booster vaccination highlights the need for further research to elucidate the impact of vaccination status on treatment outcomes. Healthcare systems must prioritize efforts to address barriers to antiviral therapy utilization and promote widespread coverage of booster vaccination to optimize the management of high-risk COVID-19 patients and reduce the burden of severe illness and mortality.




Comments (0)