
Remember me

In this study, the decision problem was to investigate the cost effectiveness of daridorexant according to its indication and treatment positioning. Cognitive behavioral therapies for insomnia (CBT-I) are the only first-line therapy recommended for the management of chronic insomnia, while existing sedatives (e.g., benzodiazepines and non-benzodiazepines) are only recommended for short-term use (<1 month). Daridorexant is the first DORA and pharmacological treatment recommended in the UK [21] and Europe [19] for the treatment of chronic insomnia. The positioning for daridorexant in primary and secondary care for long-term insomnia is as follows:
1.For treatment-experienced patients who have already completed standard of care including pharmacotherapy, daridorexant can be an alternative option.
2.For treatment-naïve patients who failed to respond to digital or face-to-face CBT-I, daridorexant may be administered as a second-line treatment.
3.Where digital or face-to-face CBT-I is inaccessible, or where a patient is unable to follow CBT-I steps, or refuses CBT-I, daridorexant may be administered as an alternative first-line treatment.
4.When longer-term management of insomnia symptoms (i.e., beyond 4 weeks) is required, daridorexant may be administered as maintenance treatment.
5.When a patient is awaiting access to CBT-I or referral to a sleep specialist, daridorexant may be administered to provide rapid symptom relief.
Given its positioning and indication, the relevant model comparator for daridorexant in this decision problem was placebo (a proxy for ‘no treatment’) in agreement with the National Institute for Health and Care Excellence (NICE) technology appraisal final scope [21]. This model comparator was also reinforced by the fact that the daridorexant 12-months clinical trial program was based on a direct comparison with placebo only. Key model features are summarized in Table 1 and further detailed throughout the Materials and Methods section.
Table 1 Overview of the cost-effectiveness model of chronic insomnia2.1 Key Clinical ParameterThe clinical outcome driving the model is the Insomnia Severity Index (ISI) [22, 23], a well-established, patient-reported outcome measure and an exploratory endpoint in the daridorexant phase III clinical trials. The ISI captures both patient-perceived insomnia severity and impact on daytime functioning and has been validated as a treatment response metric for insomnia patients [22, 24]. It consists of seven questions on a 0–4 response scale that reflect current (i.e., the last month) insomnia problems. The total score reflects the severity of insomnia, where a score of 0–7 indicates no clinically significant insomnia, 8–14 subthreshold insomnia, 15–21 clinical insomnia (moderate severity), and 22–28 clinical insomnia (severe).
2.2 Data SourcesTwo principal data sources were used to develop the model: the daridorexant 50 mg clinical trials consisting of a 12-week phase III registration study (study 301: ClinicalTrials.gov identifier NCT03545191) [25, 26] and its 40-week treatment period, double-blind, extension study (study 303: NCT03679884) [27], and a complementary observational data set from the National Health and Wellness Survey (NHWS) [28].
2.2.1 Daridorexant Clinical Trial Program2.2.1.1 Phase III Confirmatory Trial (Study 301)Study 301 was a multi-center, randomized, double-blind, placebo-controlled, parallel-group phase III trial [25, 26, 29]. Adult subjects (aged ≥18 years) with insomnia disorder but without insomnia-related comorbidities were randomized in a 1:1:1 ratio to daridorexant 25 mg, 50 mg, or placebo taken once daily in the evening for 12 weeks (84 ± 2 days) followed by a 7 ± 2 days, single-blind, placebo run-out period. The primary endpoints were the change from baseline in wake time after sleep onset (WASO) and latency to persistent sleep (LPS) by polysomnography at months 1 and 3. The secondary endpoints were the change from baseline in self-reported total sleep time (TST) and the sleepiness domain score of the Insomnia Daytime Symptoms and Impacts Questionnaire (IDSIQ) at months 1 and 3.
The ISI [22, 23] was an exploratory endpoint measured at baseline, day 28 (week 4), and day 84 (the end of the double-blind 12-week period).
The Sheehan Disability Scale (SDS) [30], a generic measure of disability and functional impairment (see Sect. 2.4.4), was also measured at baseline, day 28, and day 84.
Of note, study 302 (NCT03575104), an identically designed contemporaneous study that assessed daridorexant 10 mg and 25 mg [25, 26, 31], was not considered in this cost-effectiveness analysis beyond its contribution to recruitment for study 303 because the recommended dose of daridorexant is 50 mg.
2.2.1.2 40-Week Extension Study (Study 303)Study 303 was a multi-center, double-blind, parallel-group, randomized, placebo-controlled, extension of studies 301 and 302. Subjects who had completed the 12-week double-blind treatment plus the placebo run-out and were willing to participate were eligible to enroll. Subjects who had received daridorexant in study 301 or 302 were assigned the same dose (i.e., 10 mg, 25 mg, or 50 mg), whereas subjects who were originally randomized to placebo were re-randomized to placebo or daridorexant 25 mg in a 1:1 ratio [27, 32]. The treatment phase ran from informed consent (Visit 1) to week 40 (Visit 5), followed by a 30-day safety follow-up period, which included a 7-day, single-blind, placebo run-out. Visit 1 was performed on the same day as the end of treatment of the 301 or 302 study, after the placebo run-out assessments had been completed (7 ± 2 days), or as an independent visit within a maximum of 7 days after treatment end. The primary objective was to assess the long-term safety and tolerability of daridorexant. Along with safety parameters, ISI and SDS instruments for each subject were assessed at weeks 14, 27, and 40.
2.2.2 National Health and Wellness SurveyThe NHWS is a large, nationally representative, cross-sectional, self-administered, internet-based questionnaire of adults (aged ≥18 years) in the US, UK, France, Germany, Italy, Spain, and Japan [28]. It is designed to reflect the general population of each country surveyed, with potential respondents recruited through an existing, general-purpose, web-based consumer panel. All subjects completed the generic HRQoL instrument (EQ-5D), the Work Productivity and Activity Index (WPAI) [33], and answered questions on their health care resource use (HCRU) (i.e., general practitioner [GP] visits, emergency room [ER] attendances, and hospital inpatient [IP] stays). The WPAI captures two components of work productivity: absenteeism and presenteeism. Absenteeism refers to unplanned absences at work (here due to insomnia). Presenteeism, or working while sick, is the act of employees continuing to work despite having reduced productivity levels. Subjects self-reporting insomnia were administered insomnia-specific questions, including the ISI, thereby creating a data source that would allow mapping between the ISI and other measures of interest for the economic model.
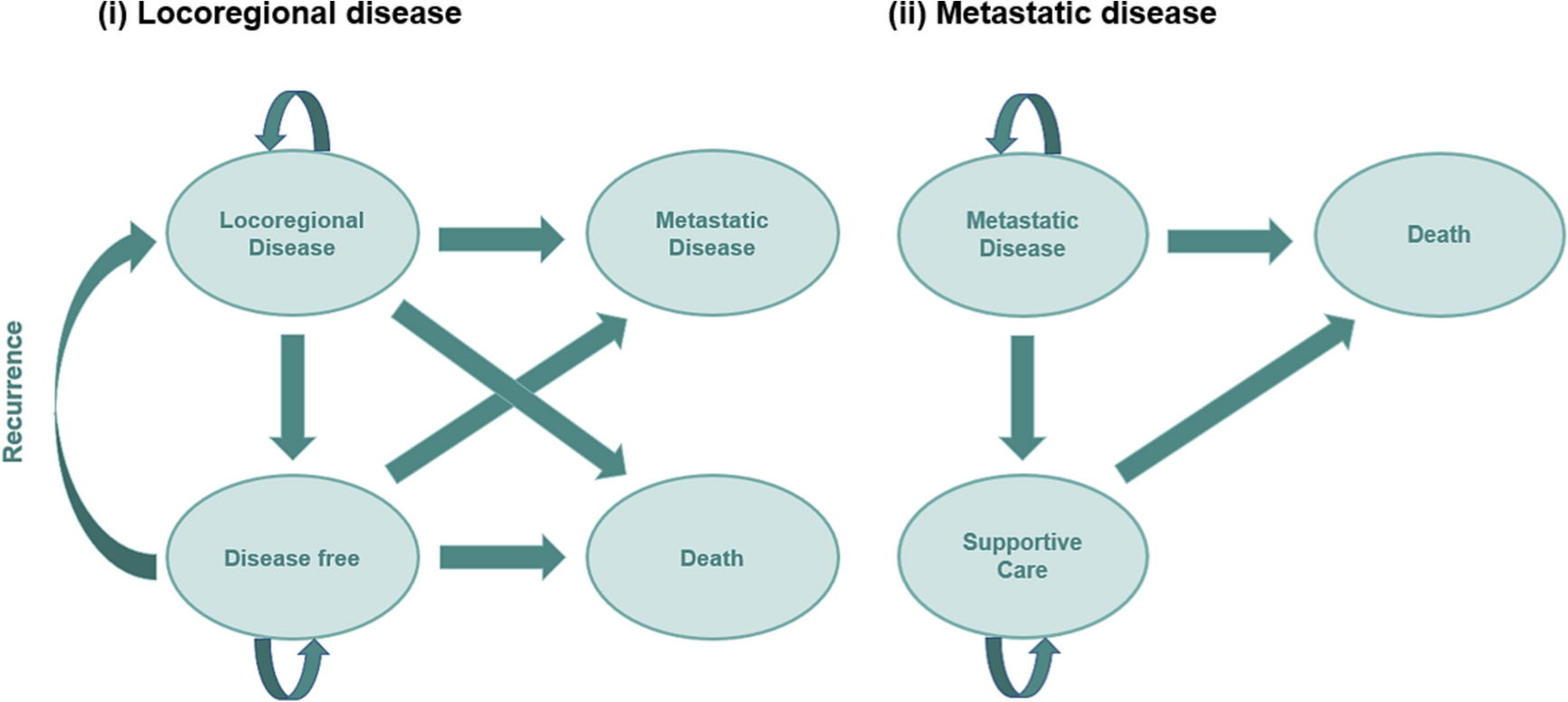
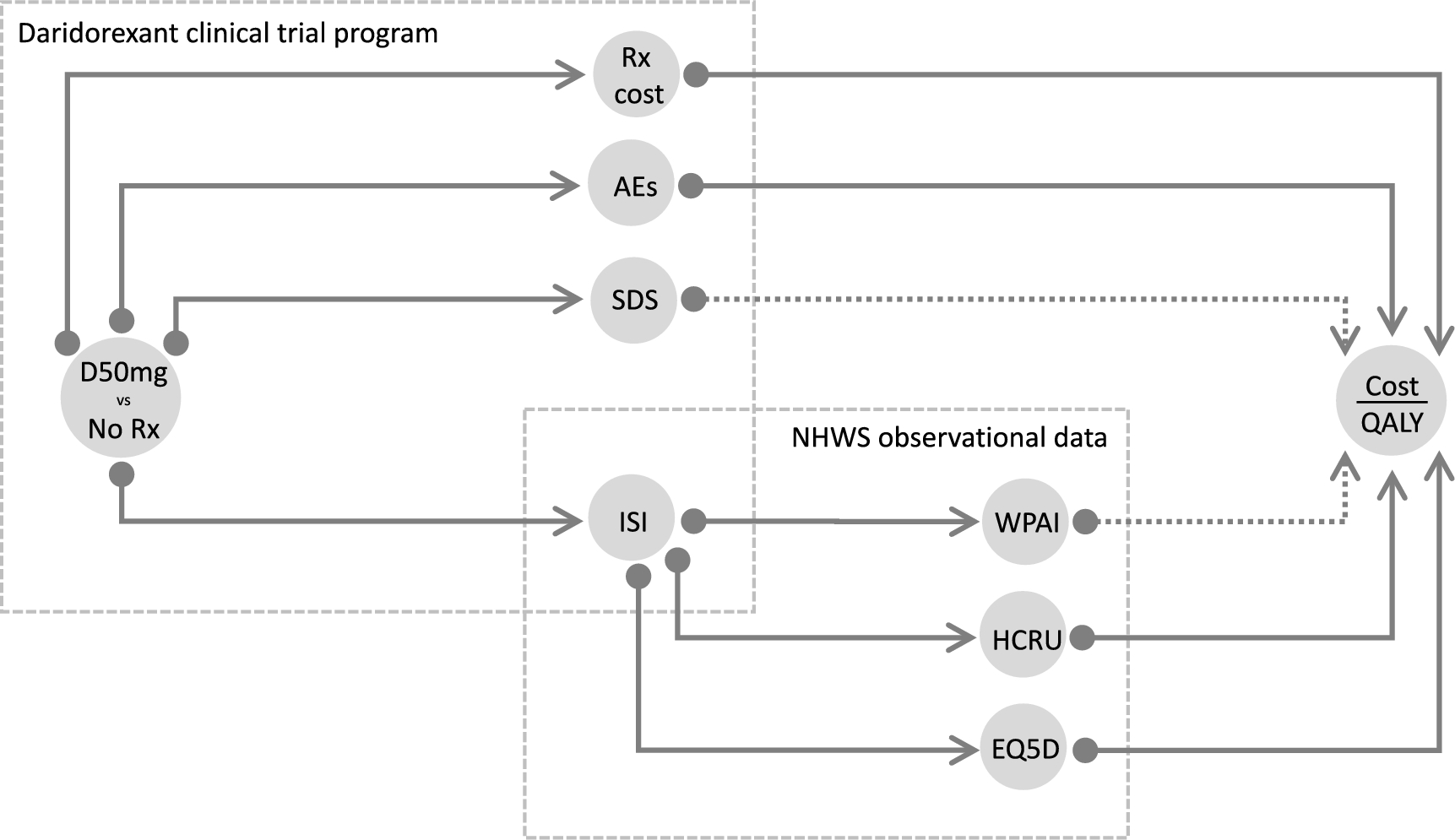
2.3 Cost-Effectiveness Model OverviewThe model structure is illustrated as pathways in Fig. 1 and shows that clinical trial data was used for the direct estimation of treatment (daridorexant 50 mg or placebo) effect on ISI, AEs, and productivity losses (SDS). This provided an estimate of the number of days on treatment at a cost of £1.40 per day. The impact of treatment on EQ-5D, WPAI, and HCRU was captured indirectly via ISI using the external data source, NHWS.
Fig. 1
Schematic of the structure of the 12-month model for daridorexant. AEs adverse events, D daridorexant, EQ-5D EuroQoL 5-dimensions, ISI Insomnia Severity Index, HCRU health care resource use, NHWS National Health and Wellness Survey, QALY quality-adjusted life-year, Rx treatment, SDS Sheehan Disability Scale, WPAI Work Productivity and Activity Index
The pathways from treatment to SDS (measured directly) or WPAI (estimated indirectly via ISI) to cost effectiveness are shown as a dotted line in Fig. 1, as the incorporation of productivity losses in the calculation of cost effectiveness is controversial, and guidance on this varies by jurisdiction. For example, in the UK, the NICE reference case excludes productivity costs [34].
As the daridorexant clinical trial program was based on a 12-week confirmatory trial (301) and its 40-week extension study (303), we chose a 12-month timeframe for the base case rather than extrapolating to patient lifetimes. We consider this as an appropriate time horizon for several reasons. First, no mortality effects for insomnia treatment are assumed; therefore, the only impact is on HRQoL (as measured by the EQ-5D). Second, daridorexant has a quick onset and short half-life, suggesting that treatment effect is gained (and lost) within a short period of time [35, 36]. This statement is also supported by the significant sleep improvement seen after days 1 and 2 in the phase II trial [35, 36] and the rapid loss of efficacy seen during the placebo run-out period of study 301 [25, 26]. Lastly, the labeling for daridorexant suggests that the appropriateness of continued treatment should be assessed within 3 months and periodically thereafter.
Adopting a 12-months timeframe allows the model to capture important aspects of treatment discontinuation, which can have both negative (dropout unrelated to outcome) and positive (dropout among subjects with less treatment benefit or safety problems) consequences for the estimated cost effectiveness. However, given indirect evidence linking insomnia to long-term problems, a lifetime timeframe could be explored on the potential long-term benefits of daridorexant on overall mortality through a reduction in road traffic accidents, cardiovascular stress, neurodegenerative diseases (e.g., Alzheimer’s disease), mental health disorders (e.g., anxiety and depression), and falls [37,38,39,40,41,42,43,44,45,46,47,48,49]. Since there is some indirect epidemiological evidence for these long-term effects, we examine separate scenarios exploring the potential long-term cost effectiveness of daridorexant when the long-term impact on general mortality is included (see Sect. 2.7).
2.4 Daridorexant Clinical Trial Program Evidence2.4.1 Impact of Daridorexant on Insomnia Severity Index (ISI) ScoreThe relationship between ISI scores at weeks 4 and 12 (study 301) was modeled using seemingly unrelated regression (SUREG) [50]. Although seemingly unrelated, the correlation structure between the regression for each time point is captured, and a joint covariance matrix is provided for all coefficients, which provides the necessary information for the probabilistic sensitivity analysis. For study 303, the aggregate data on ISI from the Clinical Study Report (CSR) [32] were used.
In addition to this ISI analysis submitted to NICE and the Scottish Medicines Consortium, an alternative mixed effects model, fitting data from both studies, was performed. This model is reported in full in the Supplementary Materials (see electronic supplementary material [ESM]) but did not form part of the submission to UK reimbursement authorities.
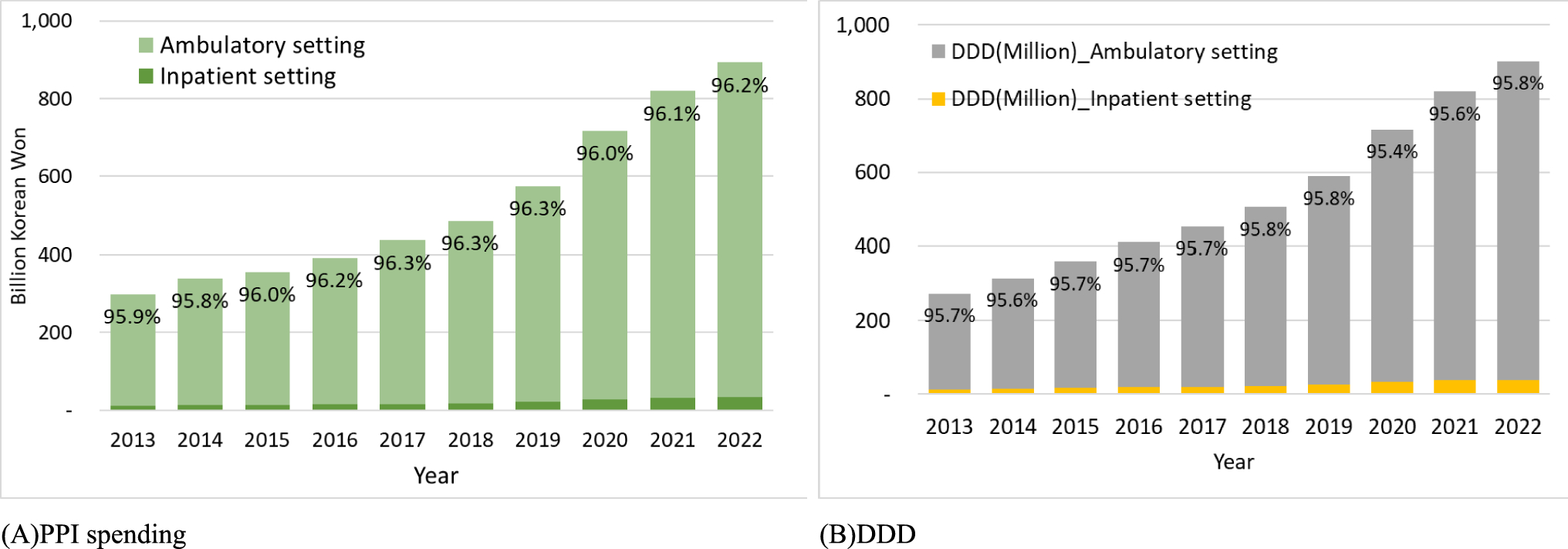
2.4.2 Treatment DiscontinuationTreatment discontinuation was based on the discontinuation rates observed in the clinical trial program. Among the 1684 subjects who completed study 301 and were given the option to continue (or not) into the extension study, 880 (52.3%) decided to do so. However, the reasons for non-participation were not reported. The proportion of subjects who discontinued was higher in the 303-extension study than in the phase III 301 study, where discontinuation rates were low (see table in Fig. 2).
Fig. 2
Total Insomnia Severity Index (ISI) scores in subjects treated with daridorexant 50 mg (D) or placebo (PLA) from the clinical trial program (studies 301 and 303). The modeled profile is represented by the solid lines connecting the studies. The dashed lines show the total ISI scores at week 13 in subjects who progressed to study 303 after the 1-week placebo run-out. The sample size contributing to each data point at weeks 0, 4, 12, 13, 26, 39, and 52 are listed in the table. The treatment effect of daridorexant on ISI is highly significant both at 1-month and final (3-month) follow-up in study 301 (Table S3 of the electronic supplementary material). The PLA group in study 303 comprises subjects from study 301 and 302
For the 804 subjects who entered study 303, the proportion of subjects who completed the double-blind treatment period was higher in the daridorexant 50-mg arm (67.9%) compared with the placebo arm (60.9%). As the reasons for treatment discontinuation were recorded, we know that twice as many people dropped their treatment due to lack of efficacy in the placebo arm (22.7%) compared with the daridorexant 50-mg arm (9.5%) (Table S1 details reasons for premature study treatment discontinuation during the double-blind period of study 303, see ESM). These data show a differential drop-out in favor of daridorexant versus placebo, which would be due mainly to the lack of placebo efficacy.
2.4.3 Adverse Events of DaridorexantThe safety of daridorexant was evaluated in the clinical trial program [19]. The label for daridorexant 50 mg identifies headache and somnolence as potential side effects of treatment and notes that these were not significantly more frequent than placebo in the registration trials.
To assess the potential impact of AEs on the cost effectiveness of daridorexant, we included an indication of the likely cost and HRQoL impact of all AEs reported in either study 301 or 303 that occurred with >2% frequency (the arbitrary cut-off adopted in the clinical study report).
2.4.4 Impact of Daridorexant on the Sheehan Disability Scale (SDS)The SDS [30] is a validated 5-item patient-reported outcome measure. It assesses functional impairment in work/school (item 1), social life (item 2), and family life/home responsibilities (item 3), measured visually as a horizontal line marked with numbers (0–10) and verbal anchors (0 = not at all; 1–3 = mildly; 4–6 = moderately; 7–9 = markedly; 10 = extremely). It also records the number of days of work/school missed in the past week (item 4) and the number of days underproductive in the past week (item 5). A measure of absenteeism comes directly from item 4, and an equivalent number of days lost due to presenteeism can be obtained from (item 1)/(10*(item 5)) [51] since (item 5) gives the number of days unproductive and (item 1)/10 gives a weight to the level of productivity on those days such that a score of 0 on item 1 would give 0 unproductive days and a score of 10 on item 1 would weight all days in item 5 as completely unproductive.
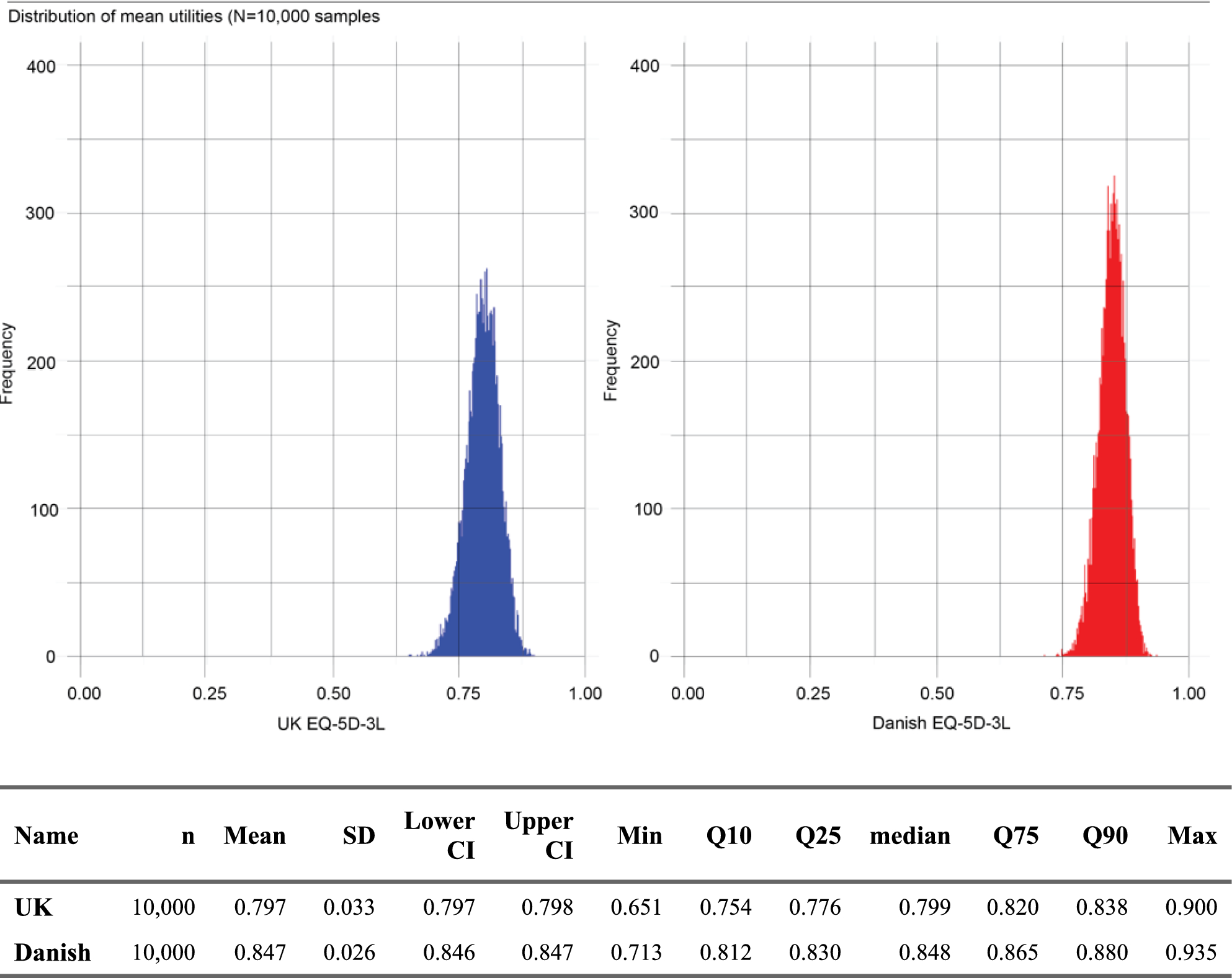
2.5 National Health and Wellness Survey (NHWS) Evidence2.5.1 Impact of ISI on UtilityA novel mapping algorithm [52] was used to derive EQ-5D-3L utilities converting EQ-5D-5L questionnaires using the Hernández-Alava et al. 2022 crosswalk algorithm [53] from ISI scores based on the NHWS cross-sectional survey. This new mapping, developed according to ISPOR task force guidance [54], not only draws its strengths from the use of a large international dataset but also incorporates adjustment variables (including sociodemographic and general health characteristics) to reduce the effects of confounders. In the base case, a generalized linear model (GLM) was used to create the mapping function. This base case model was compared with an alternative Adjusted Limited Dependent Variable Mixture Model (ALDVMM) [55] in a scenario analysis. Although the ALDVMM approach had a slightly better fit to the data, it was less parsimonious, involving five times as many parameters as the GLM used in the base case [52].
2.5.2 Impact of ISI on Health Care Resource UseThe association between direct HCRU categories (GP visits, ER attendances, IP stays) and ISI was calculated from the NHWS data using the GLM, with a negative binomial distribution family and a log link. Unit costs (base year of costing 2020/21) of £39.23 for a GP visit [56], £184.62 for an ER attendance [57], and £996.29 for an IP day [57] were applied to predicted resource counts to estimate the total health service cost.
As the NHWS data did not include two main categories of HCRU (outpatient [OP] visits and concomitant medications), a simple inflation factor was introduced to the model. In an analysis of health care costs of insomnia in the US, Wickwire and colleagues found that OP visits and prescription costs made up 27% of total health service costs [58]. In order to adjust for these missing costs in the NHWS data, the total predicted costs were inflated by 1/(1−0.27)×100%.
2.5.3 Impact of ISI on Work Productivity and Activity Index (WPAI)As the NHWS dataset included the administration of the WPAI, we examined the effect of insomnia on work productivity. The WPAI consists of six questions relating to (1) current employment; (2) hours missed due to health problems; (3) hours missed for other reasons; (4) hours worked; (5) the degree to which health problems affected productivity while working (on a 1–10 VAS scale); and (6) the degree to which health problems affected productivity for unpaid activities (on a 1–10 VAS scale) [33, 59]. Percentage absenteeism was calculated from the following formula (where Q# relates to the question number given above) as Q2/(Q2+Q4)×100% for subjects who were currently employed, and percentage presenteeism was calculated as Q5/10×100% for subjects who were currently employed and had worked in the past 7 days.
In separate models, the percentage of absenteeism and presenteeism formed the response variable in a binomial family, log-link GLM, with ISI as an explanatory variable. Percentage absenteeism as a function of ISI was then costed utilizing the median annual wage rate of £25,971 [60]. Percentage presenteeism was applied as a weighting to the percentage of time that subjects were present at work (i.e., to the 1 − percentage absenteeism) and was also costed using the median annual wage rate.
2.6 Cost Effectiveness, Parameter Estimation, and Uncertainty AnalysisPoint estimates for all model parameters were included in the model to estimate the incremental cost effectiveness of daridorexant 50 mg compared with standard of care (sleep hygiene) plus placebo. Incremental costs and incremental quality-adjusted life-years (QALYs) are presented separately from incremental cost-effectiveness ratios (ICERs). Uncertainty estimates for modeled quantities were obtained by propagating input parameter uncertainty through the model using Monte Carlo simulation (probabilistic sensitivity analysis).
Where input parameters are estimated statistically from either of the two datasets, expected values and standard errors are used for the point estimates and uncertainty, respectively. Further, where these parameters are jointly estimated from a statistical GLM, the correlation between input parameters is captured through the covariance matrix for the model and the resulting Cholesky decomposition matrix [61]. For unit costs, the standard error for probabilistic analysis was assumed to be 10% of the point estimate. Uncertainty in output parameters is illustrated on the cost-effectiveness plane and as confidence intervals.
ESM Table S2 contains a full set of input parameters for the 12-month model and information on the distributions used for probabilistic analysis. Probabilistic analyses were based on 1000 simulations.
2.7 Exploratory Lifetime ModelAlthough the justification for using a 12-month model was made in Sect. 2.3, we also noted the possible long-term impacts of improving sleep. Since it is possible that patients may stay on daridorexant for more than 12 months, we produced an illustrative lifetime model that allows extrapolation of treatment to a lifetime time horizon. In doing so, we included the following additional elements for the long-term model: potential mortality effects of better sleep estimated from the epidemiological literature [48]; an additional yearly dropout rate parameter; the inclusion of a ‘waning’ parameter to explore what happens if the effectiveness of treatment diminishes over time; inclusion of an additional GP visit in the long-term model to ‘challenge’ long-term treatment with the associated assumption that patients for whom treatment effect has waned will not restart treatment; and discount rates for costs and effects occurring beyond 12 months (both 3.5%) (see ESM Table S2 for additional lifetime model parameters). According to the labeling, ‘challenge’ was defined as a periodical review by the treating physician to assess the appropriateness of pursuing the long-term use of daridorexant 50 mg. Note that our longer-term model does not model the separate impacts of the possible impacts of insomnia identified in Sect. 2.3. Rather, we assume that the mortality impacts identified in the literature [48] are an amalgam of the individual-specific effects on mortality. Of course, this means that we are neglecting the non-fatal event impacts on HRQoL in the long term.
Comments (0)