
Remember me
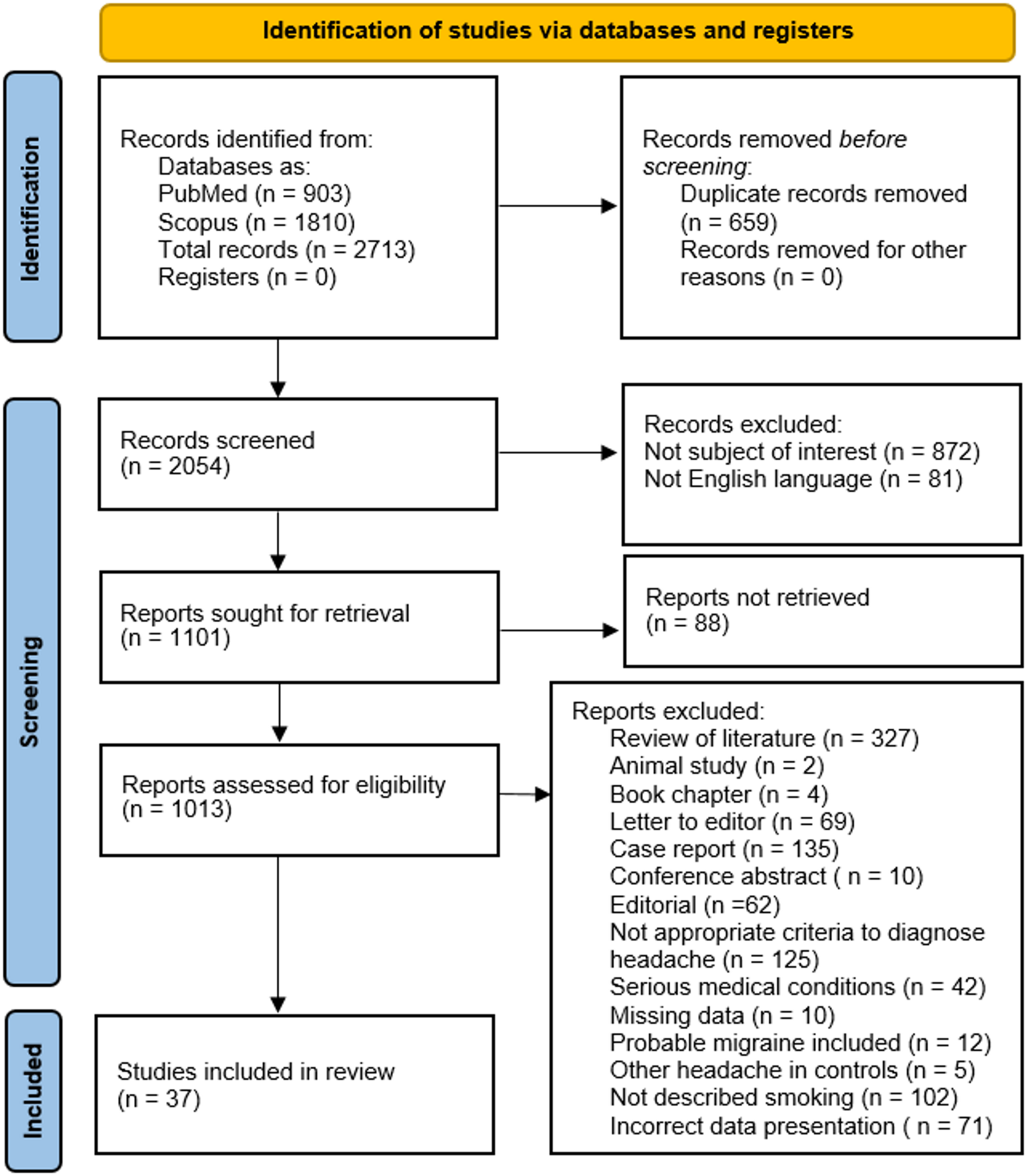
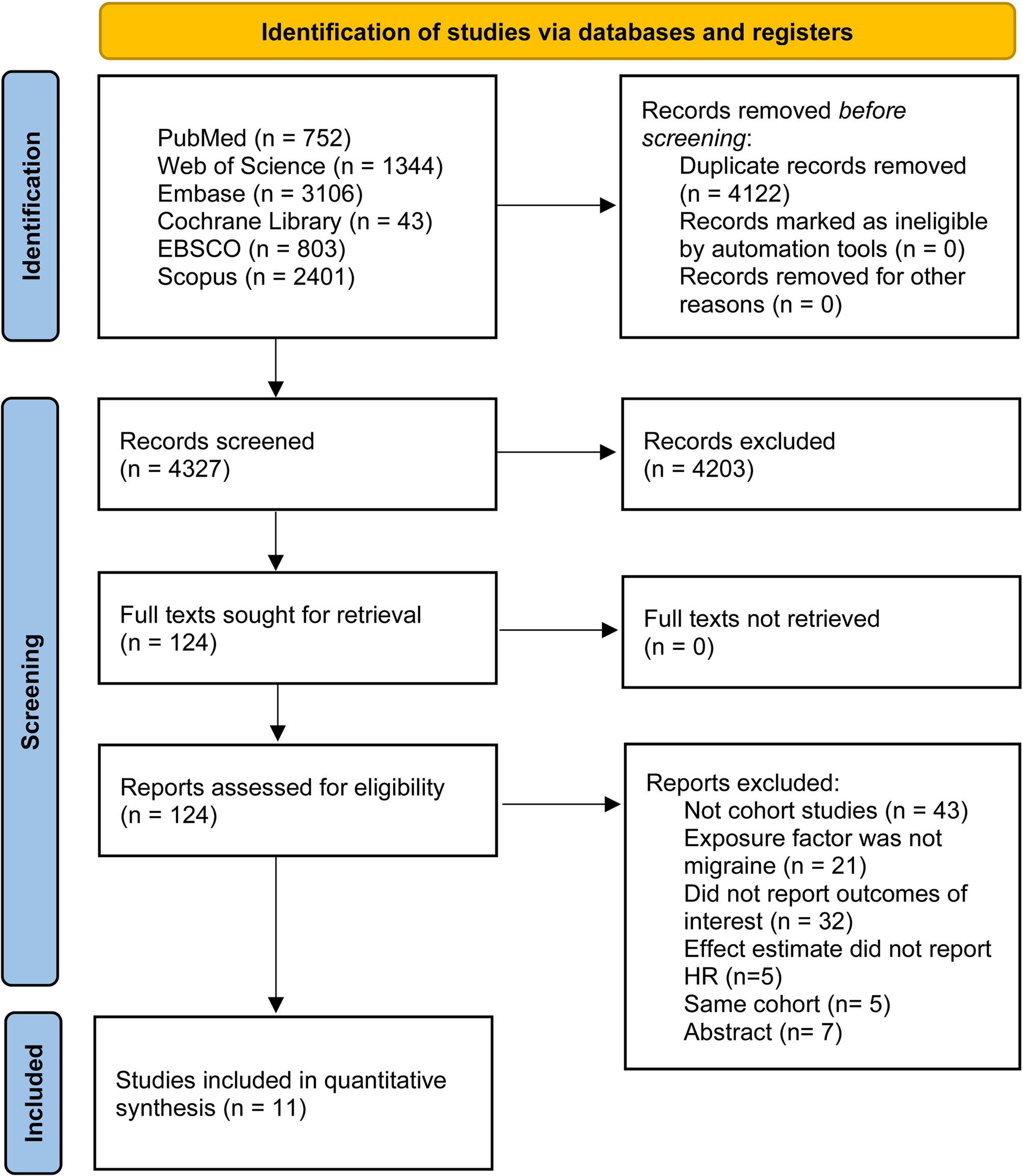



There were 2,713 search results in PubMed and Scopus. Of these 2,713 papers, there were 659 duplicates. After the duplicates were removed, the remaining 2,054 were screened by abstract and title. Next, there were 81 non-English studies, and 872 were articles not relevant to the subject of our study. Among the remaining 1,101 articles, 88 were not available to be retrieved. Of the potentiall eligible reports, there were 327 reviews, two animal studies, 4 book chapters, 69 letters to editors, 135 case reports, ten conference abstracts, and 62 editorials. In the rest of the articles, there were other reasons for exclusion such as inappropriate criteria for headache diagnosis (125 articles); in 42 papers, headache diagnosis and smoking data were for serious medical conditions; in ten, there was missing data; in 12, probable migraine diagnosis was conflated with migraine diagnosis; in five, control groups contained other types of headaches; in 102, smoking was not described according to inclusion criteria; 71 articles presented data incorrectly. Finally, 37 studies were included in the presented systematic review. Details of the steps in the selection process are shown in Fig. 1.
Fig. 1 Study characteristics
Study characteristicsThirty-seven studies were included, and these came from many countries; that is, one from Egypt [12], two from the Netherlands [20, 21], eight from the USA [22,23,24,25,26,27,28,29], two from Brazil [30, 31], two from South Korea [32, 33], four from Italy [34,35,36,37], three from Taiwan [38,39,40], two from Turkey [41, 42], two from China [43, 44], two from Germany [45, 46], and individual reports was from Iran [47], France [48], Norway [49], Spain [50], Syria [51], Greece [52], Ukraine [53], Denmark [54], and India [55]. The studies involved 24,502 participants. The most common methods to diagnose headache were ICHD criteria. Smoking was assessed in different ways, such as interview, questionnaire, or both methods combined. Different categories of smoking were utilized in the studies such as active smokers, former smokers, and never-smokers; current smokers, former smokers, and never-smokers; all smokers, current smokers, and past smokers. Some studies provided additional smoking group characteristics including amount (defined as cigarettes per day or packets or packyears), duration (years of smoking or packyears) or smoking group categorization such as mild, moderate, or heavy smoking. Twenty-seven of the 37 studies described migraine [20,21,22,23, 25,26,27,28,29,30,31, 33, 35,36,37,38,39, 41, 42, 44, 45, 47, 49, 50, 53, 55], five studies showed MwoA and MwoA [21, 35, 39, 42, 49], four studies examined smoking in TTH [30, 40, 46, 52], and nine studies were about smoking in CH [12, 24, 32, 34, 36, 40, 43, 48, 54].
Twenty-two out of 37 studies contained comparison groups marked as “control group” besides groups with primary headaches [20, 21, 26,27,28,29,30,31,32, 34, 35, 39, 41, 44, 45, 47, 49,50,51,52, 54, 55]. However, in seven out of these 22 studies, comparison group was not clearly described as patients without any headache or there was just presented as the control group involving patients with other types of headaches (primary or secondary), therefore in order to avoid potential bias risk of mixing patients with other headaches and patients without any headaches, only prevalence of smoking in primary headaches was extracted from these 7 articles [20, 26, 29, 31, 47, 50, 51]. Additionally, if covariates such as age, sex, year of publications needed for meta-regression in calculation of association between smoking and primary headaches could not be simply extracted, this study was only involved in the prevalence estimation [42, 45]. Finally, 14 studies were used to estimate the association between primary headaches and smoking [21, 27, 28, 30, 32, 34, 35, 39, 41, 44, 49, 52, 54, 55]. From all 37 studies [12, 20,21,22,23,24,
Comments (0)