
Remember me
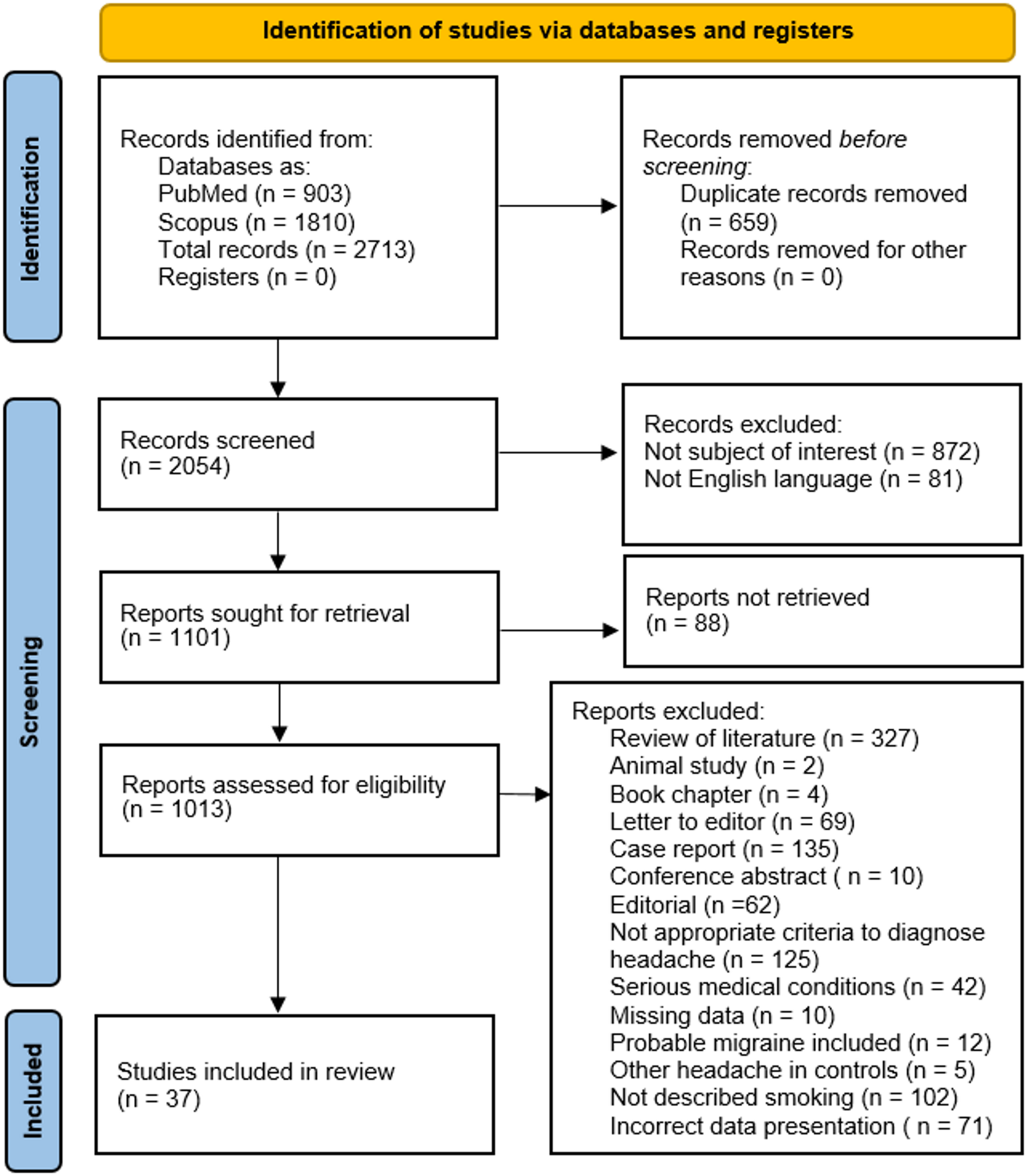
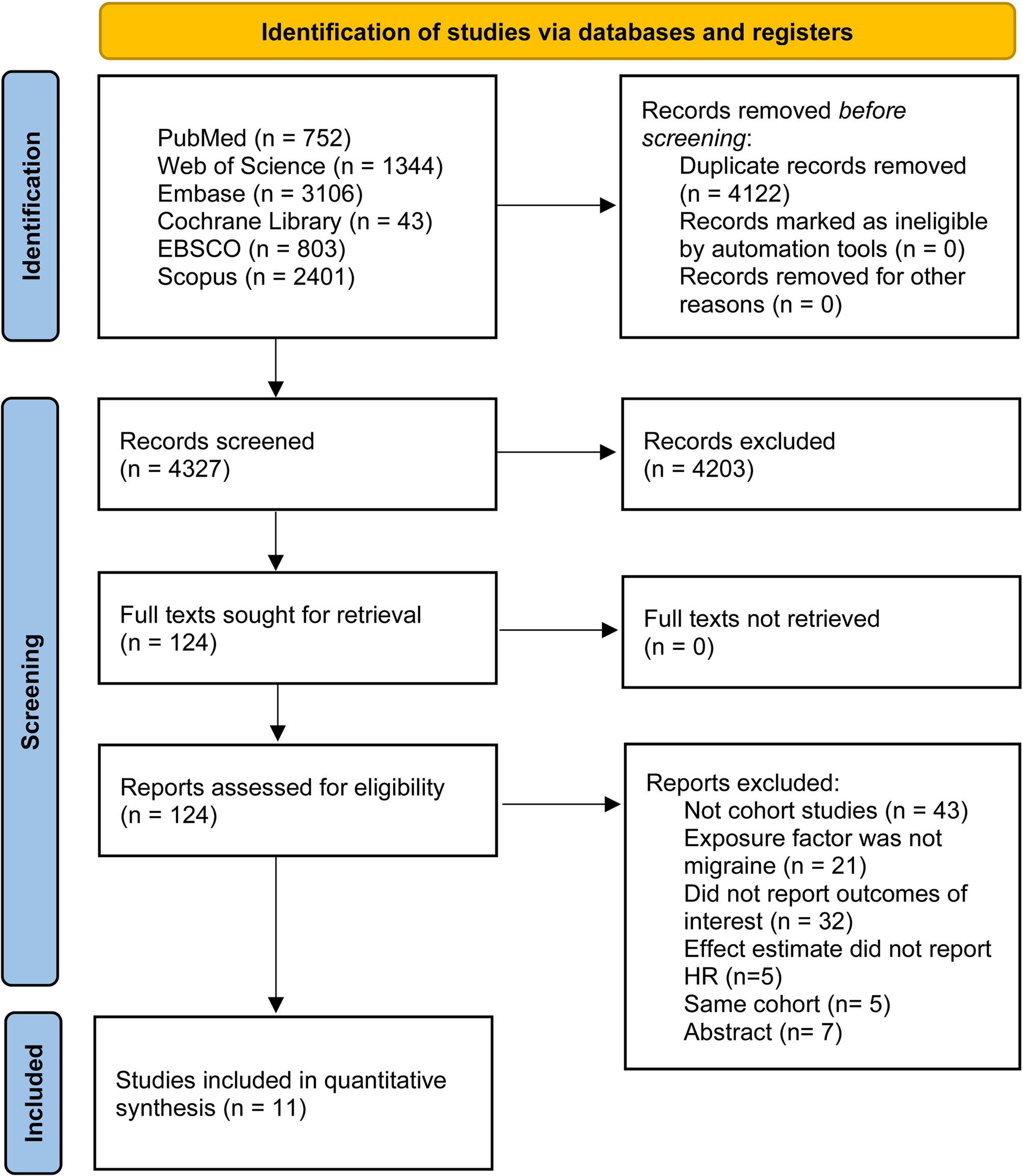



The initial search of six databases (PubMed, Embase, EBSCO, Scopus, Web of science and Cochrane Library) yielded 8,449 articles. A total of 124 studies received full-text screening, after excluding 113 studies, 11 studies were finally included. Figure 1 displays the PRISMA flowchart for detailed research selection.
Fig. 1
Flow diagram of study selection
Study characteristicsEleven cohort studies [24,25,26,27,28,29,30,31,32,33,34] including 6,691,588 controls and 272,765 migraine patients, fulfilled our inclusion criteria (three of the studies had overlap of cohorts, study with the largest cohort sizes was calculated). The publication data of the included articles were from 2014 to 2024, 6 studies were conducted in Europe [24, 26, 28, 30, 31, 33], 4 studies were conducted in East Asia [27, 29, 32, 34], and 1 [25] in USA. All of the studies included both genders. For control cohorts, 6 studies [24, 27,28,29,30, 32] compared cases to non-migraine controls, 3 studies utilized non-headache as the control group [25, 26, 31], and 1 study [33] included non-migraine, stroke, or epilepsy, and 1 study included non-primary headache disorders [34]. All studies used the appropriate diagnostic criteria to identify people with migraine, 7 studies [25,26,27,28,29, 31, 32] reported on migraine aura status. Of the 11 studies included, patients had no cognitive decline or dementia at baseline. Of the outcome indicators, 7 studies [25, 27, 28, 30, 31, 33, 34] reported all-caused dementia, 4 studies [24, 27, 29, 30] reported AD, 5 studies [26, 27, 30, 32, 34] reported VaD. All studies reported the effect measures using HR and all studies performed multivariate analyses, adjusted for at least age and sex, the majority of the studies adjusted for comorbidities, including hypertension, heart disease, stroke, hyperlipidemia and diabetes mellitus. The detailed study characteristics are shown in Table 1.
Table 1 Characteristics of the included studiesMethodological qualityEvery cohort study had NOS scores of more than seven, indicating high quality. In the comparability domain, due to the use of matched controls, 5 studies [24, 27, 28, 30, 34] demonstrated a low risk of bias. In the outcome domain, 3 studies [24, 30, 33] had a risk of bias due to inadequate follow-up data (Table 2).
Table 2 Methodological quality assessment results of the included studiesMeta analysis of the all-cause dementia risk in migraineA total of 7 studies [25, 27, 28, 30, 31, 33, 34] that reported the risk of all-cause dementia in migraine patients were included in the calculation of pooled HR. Given the extremely high heterogeneity (I2 = 84.5%) among the studies, a random-effects model was employed. According to the result, migraine substantially raised the chance of developing all-cause dementia (HR = 1.26; 95% CI = 1.09–1.46) (Fig. 2). Sensitivity analysis showed that, excluding none individual study altered the overall direction of effect (Supplementary Fig. 1.A). Funnel plot, Begg’s test and Egger’s test indicated no evidence of systematic asymmetry on examination (Supplementary Tables 2 and Fig. 2.A). Subgroup analysis on region showed that Asian migraine patients had an increased risk of all-cause dementia (HR = 1.59; 95% CI = 1.04–2.42, I2 = 91.8%) (Table 3). Through subgroup analyses by the type of migraine, it was found that migraine with aura had an increased risk of all-cause dementia and reduced statistical heterogeneity (HR = 1.22; 95% CI = 1.03–1.44, I2 = 38.6%), but migraine without aura was not (HR = 1.13; 95% CI = 0.94–1.37, I2 = 74.9%). Subgroup analysis according to different diagnostic criteria for dementia showed that, migraine patients had an increased risk of all-cause dementia in studies that used ICD criteria (HR = 1.38; 95% CI = 1.18–1.62, I2 = 82.2%). Heterogeneity between studies using Diagnostic and Statistical Manual of Mental Disorders (DSM) criteria decreased, but the risk of all-cause dementia was not significant (HR = 0.99; 95% CI = 0.83–1.18, I2 = 23.8%). Subgroup analysis by gender showed that the result was only significant in women (HR = 1.28; 95% CI = 1.12–1.47, I2 = 62.6%). Migraine significantly increased the risk of all-cause dementia in high quality studies (NOS score was 9) (HR = 1.51; 95% CI = 1.23–1.85, I2 = 85.8%) and studies with sample sizes more than 2000 (HR = 1.29; 95% CI = 1.13–1.46, I2 = 70.5%). The high risk of all-cause dementia in migraine groups was observed when the studies used non-migraine controls (HR = 1.29; 95% CI = 1.13–1.46, I2 = 70.5%). The meta-regression analysis showed that region (P = 0.912), migraine type (P = 0.661), diagnostic criteria for dementia (P = 0.109), gender (P = 0.538), NOS score (P = 0.101), sample size (P = 0.819), controls (P = 0.819) and mean follow-up time (P = 0.427) were not significant sources of study heterogeneity.
Fig. 2
Meta analysis of the all-cause dementia risk in migraine
Table 3 Subgroup analysis of the all-cause dementia risk in migraineMeta analysis of the Alzheimer’s disease risk in migraineFour studies [24, 27, 29, 30] reported the risk of AD. Meta-analysis showed that there was a notable difference in AD risk between individuals with migraine and the control group (HR = 1.48; 95% CI = 1.31–1.67). Substantial heterogeneity (I2 = 90.9%) was observed across studies. Sensitivity analysis showed that the I2 value decreased by 38.4% when the result of Geng [24] was not included. The study investigated the association between migraine and AD risk by analyzing data from a sample comprising 404,318 individuals, utilizing the UK Biobank dataset. Adults with migraines suffer from a significant burden of depression and/or anxiety [35], while study have found that people with depression have a higher chance of developing AD [36]. This study did not adjust for depression, hyperlipidemia, Parkinson’s disease, resulting in a higher HR than the actual value. After removing this study as an outlier, migraine was still a risk factor for AD (HR = 1.32; 95% CI = 1.26–1.38) (Fig. 3). Sensitivity analysis showed the result was reliable (Supplementary Fig. 1.B). Begg’s test, Egger’s test and funnel plot indicated no significant risk of publication bias (Supplementary Tables 2 and Fig. 2.B).
Fig. 3
Meta analysis of the Alzheimer’s disease risk in migraine
Meta analysis of the vascular dementia risk in migraineA total of 5 studies [26, 27, 30, 32, 34] reported the VaD risk in migraine patients and the control group. There was no significant heterogeneity among the studies (I2 = 27.6%), and a fixed-effect model was used. The result of meta-analysis demonstrated a significantly increased risk of VaD in migraine patients (HR = 1.28; 95% CI = 1.24–1.32) (Fig. 4). Sensitivity analysis showed that the result was reliable (Supplementary Fig. 1.C). Egger’s test indicated the existence of publication bias in the included studies (P = 0.048) (Supplementary Tables 2 and Fig. 2.C).
Fig. 4
Meta analysis of the vascular dementia risk in migraine
Comments (0)