
Remember me
We interviewed 8 parents diagnosed with BD (5 mothers and 3 fathers), and 3 non-bipolar partners or ex-partners of parents with BD (1 father and 2 mothers from separate households). As shown in Tables 1 and 8 of 11 parents held graduate degrees, with most co-parenting in the same household (9 out of 11), predominantly from Southern England (7 out of 11), and all identified as white. Stakeholder participants, detailed in Table 2, included 5 charity workers or volunteers and 7 mental health professionals or social workers, providing diverse insights into supporting families affected by BD. Interviews were held via Microsoft Teams (n = 21) or telephone (n = 1), audio-recorded except for one parent who, due to mood, responded via written questions on Qualtrics. The average interview duration was 86 min for stakeholders (range: 52 to 103 min) and 95 min for parents (range: 45 to 154 min), including two parent interviews split into two sessions due to scheduling constraints. No adverse events or distressed occurred during discussions of BD communication.
Our analysis generated 74 refined codes—52 from both parents and stakeholders, 9 from parents only, and 13 from stakeholders only—distributed across themes: Theme 1 (Perceived Advantages) with 10 codes, Theme 2 (Perceived Challenges) with 11 codes, Theme 3 (Key Elements) with 29 codes, and Theme 4 (Practical Strategies) with 24 codes, with subtheme details in Supplement 2. The theme structure is robustly supported by triangulation, with most subthemes (8 of 12) incorporating perspectives from all five roles—fathers and mothers with BD, non-bipolar partners, mental health professionals or social workers, and charity workers—enhancing the findings’ reliability, while all subthemes include contributions from at least four roles.
Theme 1: perceived advantages of communication about BDParticipants highlighted several benefits of discussing parental BD, emphasising both educational and relational aspects. This communication was viewed as enhancing children’s awareness and understanding of BD, promoting their personal growth, and strengthening trust and emotional bonds within the family. These perceived advantages are explored through the following subthemes.
Subtheme 1.1: promoting understanding and reducing misconceptions in childrenParents and professionals noted their beliefs that children often form their own interpretations of parental BD, which can lead to misconceptions and fear. A father with BD explained: “They [children]… have all sorts of theories [about parental BD]… until they’re told the reality” (P07). A mental health nurse shared an example from their experiences, suggesting that without accurate information, children may become anxious and confused when trying to make sense of their parents’ unpredictable behaviours: “The children don’t actually know what’s happening [during an episode]… then they become frightened and scared of what the parents are actually doing and trying to conceptualise it for themselves” (S08).
Parents and professionals both reported that effective communication can help children understand how BD affects parental behaviour and reduces misconceptions. A family therapist noted: “It [communication] is fair to both parties… because when the child is more aware… why is my mum or my dad saying something like this? They don’t mean to say something like this” (S01). A charity worker highlighted that honesty reduces anxiety: “It’s much better to be honest (about parental BD), because then it’s not so frightening for the child” (S07). This understanding can also empower children to cope with parental mood swings and may help them avoid blaming themselves for their parents’ behaviours. As a mother with BD shared: “Often she [daughter] goes ‘it doesn’t matter… I know it’s just your mood.’… she knows it is just my illness” (P08). Furthermore, sharing information about BD may foster psychological maturity, encouraging children to reflect on their interactions with their parent with BD. Another mother with BD described how this communication enhanced her child’s empathy: “She [the child] understands everybody’s individuality… she understands some of [others’] things are not her things. So, seeing it from their perspective… I do feel like [this understanding] made them more compassionate towards not just me but everyone” (P06).
Subtheme 1.2: fostering expression and strengthening bonds in childrenParents and professionals observed that discussing BD can encourage emotional dialogue between parents and children, particularly since children may hesitate to share their emotions for fear of upsetting their parents with BD. As one mother with BD remarked: “Sometimes he [my son] doesn’t always want to say how he feels because he is worried that he’s going to affect you or upset you” (P04). A mother with BD shared her belief that fostering open communication creates a safe environment for both parents and children to express their concerns, noting that such transparency not only “gives [children] the opportunity to come and talk to me or their dad if they have anxiety over something in their lives,” but also makes it “much easier to tell them if I am in a depressive episode” (P11). A peer-support group facilitator explained that this approach helps children articulate their emotions: “They [parents with BD] would describe how they feel… they got their kids used to talking about their feelings in this way and started explaining… ‘This is how I feel today’” (S04). Professionals specifically observed that engaging in honest and supportive dialogue can also help reduce feelings of isolation, as children may feel they are the only ones who have a parent with BD. A charity worker observed: “Children in this situation feel shame… because mental illness isn’t talked about, and they think that they’re the only ones experiencing family life like this” (S02).
Parents and professionals also reported that discussing BD with children can strengthen the parent-child bond and build trust. A father with BD affirmed: “I think [talking about] it is a good thing… it definitely does help the bond because we’re able to talk about that [parental BD]” (P05). This communication may also help maintain connections in families experiencing physical separation. A peer support group facilitator recalled how one father, living apart from his daughter, used letters to bridge their communication gap: “His daughter [initially] refused to talk to him… he found it easier to communicate [through letters], explaining to her… why he’s not together with her mum, why he sometimes acts the way he does, and how he feels… I know they did exchange a few letters and he found a lot of comfort in them” (S05). However, it remains unclear how the daughter perceived these letters or what impact they had on her.
Theme 2: perceived challenges of communication about BDParticipants voiced concerns about communicating parental BD to children, particularly regarding uncertainties around what to share, when to share, and how to approach the discussion. These challenges were further complicated by fears of how children might perceive the conversation and the psychological burden it could impose. This underscores the need for thoughtful guidance to help parents discuss BD in a way that maximises benefits while minimising harm, as explored in this theme.
Subtheme 2.1: fears of placing emotional burdens on childrenBoth parents and professionals expressed concerns that sharing a parent’s BD diagnosis could confuse or distress children particularly if the conversation isn’t tailored to their age and emotional readiness. A charity worker emphasised the need for sensitivity in this process: “The child could be really upset at the end of [the conversation] or not want to take the information in. I think that depends on that child and parent relationship and how it’s sensitively conveyed” (S03). This risk became evident when one daughter appeared overwhelmed by her mother’s unplanned disclosure of past suicidal thoughts: “I was just waiting at the bus stop, and I said something about when I was suicidal and [my daughter] went ‘What?’ I hadn’t realised I hadn’t mentioned it… she was really, really shocked… oh bless her” (P08). Worries about triggering such emotional impact may heighten parental hesitation in starting the discussion. A father with BD explained: “I would not go into the ins and outs of what bipolar is… it could easily frighten them [the children]” (P07). Concerns about hereditary risks also weighed heavily on some participants. A mother with BD worried: “I would be really concerned that he [my son] might worry that he might have it [BD] and get diagnosed with a mental illness too” (P02). She also feared her postpartum diagnosis might emotionally burden her son: “I’m really concerned because of the way I was diagnosed as being a postpartum-related diagnosis, I am really concerned that [the son might] ever feel that it was his fault” (P02). Professionals specifically observed that these conversations can become more complex when both the parent and child have mental health concerns. A peer group facilitator noted: “If you’re in that situation of a parent having bipolar and their child having anxiety problems, you wouldn’t want to be a burden on the other. So often, you would not communicate what’s going on because you know that the other one is struggling” (S05).
Subtheme 2.2: self-acceptance and stigma as barriers to communicationBoth parents and professionals suggested that the way parents perceive their diagnosis influences their willingness to communicate about it. A social worker observed, “The parent’s relationship to the diagnosis… if a parent doesn’t find that diagnosis particularly helpful or they’re feeling stigmatised by the diagnosis… that informs how they might want to talk about their mental health with their children” (S09). Struggles with self-acceptance can limit openness, as a charity worker explained: “[Disclosure] is sort of like how parents feel comfortable about their own diagnosis if they accept it” (S03). Participants noted that when parents do not feel the BD diagnosis is helpful or do not recognise it, they may avoid communication altogether. One mother shared that her ex-partner refused to talk about his BD: “In terms of my kids, they have a dad that will not talk about his bipolar. It does not come up in conversation ever. He actively avoids it… it often leads to real disappointment [in children]” (P03).
Both parents and professionals expressed concern about how children might perceive their parents after discussing parental BD. Parents worried their children would see them as “something wrong” (P06), “seriously different from other dads” (P03), “weird” (S10), or “not capable of looking after [their children]” (S07). These fears could shift family dynamics, leading children to view the parent with BD as less reliable. A “well” father observed: “It [the conversation] made them [the children] very much more dependent on me. They felt that… I was the safer parent to be with” (P10). Some parents also feared their children’s reactions, as one mother with BD shared: “I haven’t really explored it [parental BD] with him [the child]… I’m a bit scared to ask him directly. You know how you feel scared of what his answer would be” (P02). Professionals noted that stigma could also extend to interactions with extended family and the community, further complicating these conversations. A social worker shared their experience of working with parents who perceived that “If I [the parent] tell my kids, then my kids are going to tell the neighbours’ kids, which means the neighbours know, and I think it’s all wrapped up in stigma” (S10).
Subtheme 2.3: uncertainty in communicating about BDBoth parents and professionals highlighted the uncertainty that parents face regarding what, when, and how to communicate about BD. A psychiatrist noted that parents often question: “How much do I tell them [children]? What do I share? How do I share?… Am I in some way contributing to their anxiety by either showing them too many of my symptoms or hiding my symptoms?” (S06). The unpredictable course of BD symptoms can make it especially challenging to answer questions like “Are you always going to be like this?” (P05), “Why are you ill?” (S06), or “Is this going to happen to me?” (P07). As a father with BD explained, the episodic nature of the disorder can complicate these conversations: “It’s a bit difficult to explain just how it’s sometimes… most of the time I’m okay, and then sometimes I’m not” (P05). A charity worker added, “The biggest struggle in the conversation [with children] was to talk about the fact that bipolar disorder cannot be fixed” (S04). Determining the right time to share information about BD is also challenging. A charity worker noted parents with BD often ask, “When they should tell [their children]” (S07). The child’s age and developmental stage seem to play a significant role, as one mother described: “When they [the children] were very little, it was really difficult to explain that [parental BD] to them to make any sense” (P03). As children grow older, parents may fear their child’s increasing awareness and deeper questions, as another charity worker observed: “[Children are] asking more questions [about parental BD] and starting to become more aware” (S03). Parents often grapple with uncertainties about BD’s heritability, as a mother with BD shared: “I think nobody really knows what the genetic links are” (P02).
Theme 3: key elements of communication about BDParticipant accounts identified four key elements of communication about BD: tailored communication, addressing children’s concerns, providing reassurance of a consistent personality and love, and preparing for future episodes. These insights are derived from participants’ lived experiences and their beliefs about what contributes to the communication process with children.
Subtheme 3.1: age-adaptive communicationBoth parents and professionals noted that discussions about BD often begin with issues relevant to children, such as changes within the family. One mother explained: “It started off as a conversation [with the children] about why we are living here? Why aren’t we still living with Daddy [who has BD]? So we first kind of tackled that… to allow her [the child] a little bit of understanding about what bipolar was… why he behaved in the way that he behaved at the time” (P03). For younger children, participants emphasised using simple, everyday language, avoiding medical terms like “psychosis” (S08), “neurochemicals and neurotransmitters” (S12), and “brain chemical imbalance” (P07). Instead, parents recommended phrases such as “I have something in my brain” (P04), “my brain doesn’t work the same” (P06), or “Papa goes up and down with his mood” (P09). As children mature, more detailed information can be introduced through online articles (P03), scientific explanations (P07), or websites about BD (P09). Participants suggested that using familiar analogies or metaphors may help explain BD to children. One mother compared the disorder and its treatment to a physical injury: “It never goes away because once you’ve broken a bone, it remains weaker than it was before… It’s like when you break your leg, you have to have medicine to manage the pain… wear a cast… to make it better” (P03). To make these explanations resonate, parents sometimes develop unique terms that fit their own context, referring to medications as “my crazy pills” (P06) or using “sleep diarrhoea” for excessive sleeping (P10), reflecting how they personalise language to better communicate with their children.
Both parents and professionals emphasised the importance of developmentally appropriate, child-friendly materials for communicating about BD. For younger audiences, a psychiatrist suggested using familiar cartoon characters: “I think it’s got to be done in their language… [like] Winnie the Pooh… if you look into it, all the characters have a mental health issue… that’s the way to present it to very young children” (S12). Storybooks were also valued for age-appropriate dialogue, with a charity worker noting: “We’re sending a resource to somebody that could sit down and have a conversation in a book with the child through a story” (S03). Mood charts were another tool to engage families: “You’re looking at the sort of zero being the really low mood, suicidal, to the mania, the psychotic… the ten… they could use it alongside the family and say, like, ‘What’s your mood today?’… It could become a resource that everybody on the fridge has a mood scan, ticks their mood each day to see how’s everybody doing” (S03). Participants also advocated for simple, practical aids like leaflets to ease the burden on parents. A peer-support group facilitator shared: “A simple tool like a little leaflet… takes the pressure off the parents… [on] how to explain it [BD] to a child” (S04). Engaging visuals were emphasised, as a nurse explained: “Something like that with lots of pictures… not like diagrams… because that then gets a bit too anxiety-provoking” (S08). However, participants acknowledged a shortage of resources for younger children. A social worker pointed out: “Books that you tend to have are written for teenagers… there’s nothing out there for littlies that says… sometimes mum might be like this” (S10).
Subtheme 3.2: addressing children’s concerns and misconceptionsBoth parents and professionals highlighted that clear, two-way dialogues may help children manage emotions like worry, guilt, and the caregiving burden associated with parental BD. Open communication was seen as key to preventing children from feeling responsible for their parents’ condition. A father with BD stated: “I always try to say that it’s not about you. I’m not depressed because of you. And that it’s not their fault, so [I’m] trying to explain the triggers without making them worry about me or blaming themselves” (P05). Addressing children’s fears about the severity of BD was also perceived as crucial by a charity worker: “They [the children] look up bipolar and see it’s got the highest suicide rate of any condition… they might think you’re going to die. Every time you go out, they might be worried about you… I think you need to face those things and decide how you are going to do it… in a very thorough way” (S07). One father discussed clarifying misunderstandings, such as confusing physical illness with BD: “The slightest hint of illness will make her [the child] very worried… if [the mother with BD] has COVID and is in bed for a day, that associates with ‘Mummy’s really depressed’,” said another father (P10). He also addressed children’s fears about inheriting BD: “[My child] thinks that if I don’t sleep well for a night, I might end up… being carted off into hospital against my will… I explained that if you have an illness called bipolar, and then you go without sleep, it can make you look like this [relapse]… if someone who doesn’t have that condition [BD] goes without sleep, they don’t have any problems” (P10). Discussing genetic risks requires reassurance, as a charity worker added: “It’s important to make that clear… you’re probably not going to have this [BD], but even if that was the case, we as a family know an awful lot about it, we can support you” (S07).
Subtheme 3.3: reassuring consistent love and personalityParents and professionals both highlighted the importance of instilling hope in children by emphasising that BD episodes are temporary and treatable. One mother explained that her son needs “someone to assure him that… it will get better… the situation, or the father [with BD]” (P09). Participants emphasised the consistent nature of parental love, as a social worker explained: “Mum’s got something going a bit kooky in her mind… it makes her do some strange things sometimes, [but it] doesn’t stop her loving you” (S10). Showing that parents continue to make efforts, even during BD episodes, may reinforce this message. A peer support group facilitator remarked: “Even when someone is down, they are there for you just in their own way and in the best that they can do that day” (S05).
Reassuring children about the continuity of personality amid BD’s impacts was perceived as essential by parents. One father observed how children may struggle to distinguish between their parent’s normal emotions and those tied to BD: “If she [the mother with BD] gets a little excited… feels a bit down, or gets cross, there will be three people in the family thinking, ‘Oh, is this the start of an illness episode?’” (P10). This blurred line between typical behaviour and BD symptoms can be confusing for children. A mother suggested helping children “recognise which elements of him [the father with BD] are driven by the bipolar and which elements of him are just him” (P03). Another mother used a nickname for her BD: “I call my bipolar Betty… it’s separate from me… a part of me, but she’s not who I am. It just made more sense to explain it to a child in that way… it’s not his mum. I’ll just say, I feel like I’m Betty. Betty’s really like taking over at the minute” (P04). This approach might help children understand that while BD affects their parent, it doesn’t define who they are.
Subtheme 3.4: preparing and supporting children for future BD episodesGiven BD’s episodic nature, both parents and professionals stressed the importance of preparing children for future episodes to foster resilience and provide a sense of control over the situation. One father with BD explained how he prepared his son for potential mood changes: “I explained to him [the son] what might happen… make sure he’s informed about how I feel and then say to him… don’t worry about it too much if I react this way, which is my illness [BD]” (P01). A charity worker advocated for proactive planning, encouraging parents to think through difficult scenarios and explain these plans to their children: “Think through scenarios that you don’t want to think about… if I go into hospital, what happens to my child… If it’s actually written down, and you explain it to them… children are not going to be so worried” (S07). A mother with BD further highlighted the need for maintaining appropriate boundaries, stating that children’s role should be supportive, not caregiving, when parents are unwell: “I never want my children to feel it’s their job to look after me” (P11).
Parents acknowledged the value of helping their children understand their emotional needs during BD episodes. A mother sought to help her children recognise and interpret their father’s needs during his BD episodes: “They need to learn to understand… when he [father with BD] is unwell… much more kind of extreme. It’s basically him saying… ‘I’m unwell, I don’t want to be bothered by you, leave me alone and let me be’, so it’s about recognising” (P03). However, a father with BD cautioned against portraying the disorder to children as something uncontrollable, urging parents to avoid “over-medicalising it, like, this is something that just happens out there, nothing can be done” (P05). Instead, he emphasised the importance of expressing his emotional needs during an episode and encouraging his children to offer simple forms of support without making them feel responsible for his care: “ It’s just giving me a cuddle, or… encouraging me to come out, or do something fun when I’m down… how the child can help you… [so they] doesn’t feel like you have to look after and end up being a carer… almost like a relapse prevention plan for both of you… ‘If daddy’s unwell, I can do this’” (P05).
Theme 4: principles of communication about BDThis theme explores strategic principles that parents with BD may apply to communicate effectively with their children. It focuses on determining the optimal timing, selecting the appropriate level of detail, and adopting a clear and interactive communication style. The theme also examines the roles that family members and professionals can play in facilitating these crucial discussions.
Subtheme 4.1: ‘how to communicate’ - transparency and two-way conversationBoth parents and professionals recognised that parents sometimes use oversimplified or vague language when sharing information about BD with children due to uncertainties about how much to share. However, they also recognised that children can sense when something is wrong, and incomplete communication may raise anxiety. A psychiatrist explained: “They [children] obviously understand something is wrong… not telling them what exactly it is, is just going to raise anxieties” (S12). Some parents, who had not understood their own parents’ illness, felt a strong motivation to be transparent with their children. One mother with BD shared: “I grew up with my mum who had schizophrenia and I, in some ways, didn’t understand her illness. So I used to look after her and felt sad for her but not fully understanding why. I never want my children to feel this way” (P11). Participants emphasised that while honesty is important, information should be delivered with sensitivity to the child’s emotional readiness and level of understanding. A charity worker noted: “I think usually honesty is the best policy, but sometimes it’s about finding the right time… finding the right words, and answering questions and being available… just to make things as non-threatening as possible… they need to understand what it is they might have to deal with” (S02).
Parents and professionals also highlighted the value of fostering a two-way conversation in which children feel safe enough to ask questions. A social worker noted: “I think it’s not just the description of what the mental health presentation is; I think it is what the parent enables in the relationship—that you can talk to me. Even though these are difficult questions, I’m here and I’m able to listen… there’s something quite reassuring in knowing that I’ve got this worry, I’ve got this concern, and if I say it out loud, my parent is going to help me sort it out and give me back some information that is reassuring… The child is able to know that it’s safe to talk about their feelings and have them validated” (S09). Participants observed that children often have questions about their parents’ BD, and it’s important for parents to address these concerns. One mother with BD shared: “They [children] have asked about my medication, like, ‘What does it do?’… And they do ask… why sometimes I do certain things and why sometimes I don’t” (P06). A father whose partner has BD added: “He [the child] asks very probing questions and just keeps going with the questions… you’ve kind of got to go with what they feel they need” (P10). Although parents might worry about providing the wrong answers or whether their children are ready for certain information, one mother shared her approach: “Have the conversation led by the children, and just answer to the best of my ability, and try not to be scared of answering difficult questions… If you’ve asked the question, then you’re old enough to listen to an answer” (P03).
Subtheme 4.2: ‘when to Communicate’– Timing and context considerationParents and professionals had varied opinions on when to communicate about BD, often influenced by the child’s ability to understand. One father with BD noted: “Being 12 and 10, they would have a fairly reasonable amount of understanding” (P07). Some parents waited for signs of maturity, as a charity worker explained: “What age should I tell them… I think that’s very individual… one [child] can be very mature at five or six, and another might not be until they’re 10” (S07). Others waited until BD symptoms became noticeable, with a mother with BD stating: “I now discuss bipolar quite openly with my children as it has an impact on everyone, not just me” (P11). Conversely, some participants felt that adults often underestimate children’s understanding. A psychiatrist shared: “Children often know more [about parental BD] than you think they know” (S06). As a result, some parents favoured early communication, tailoring explanations to the child’s level. One mother with BD likened it to sex education, saying: “They [children] are never too young, but there’s always a level you can explain it at” (P08). A partner of a father with BD added: “I would not put an age limit on it [communication]… to avoid a surprise moment later in life” (P09).
Parents and professionals identified emotional stability, preparation, and natural opportunities as key factors for effective communication. A social worker highlighted the need for stable moments for safe discussions: “The challenge is if they [parents with BD] are in a high phase or a low phase, actually that pressure on them, when you’re trying to make somebody else feel better about what’s going on for you, it’s impossible… [Disclosure is] really triggering anxiety if… they’re trying to talk to you about what’s going on for them” (S10). Careful planning was also recommended, with a charity worker suggesting: “I think an important thing is to put a lot of thought into it, you know, to really think about it and have enough time to really sit down and have a long [conversation]… Plan in your head how you can say reassuring things… like… doing an advance statement or directive” (S07). Participants noted that natural occasions, like media or daily interactions, could ease the conversation. A charity worker shared: “We’d seen the character on EastEnders, and they [children] said… ‘What’s the matter with her [the character with BD]?’ and we talk about it [BD]… seeing them on the screen gives you an opportunity to bring the subject up,” one charity worker observed (S07). Schoolwork also provided openings for discussions, as one father with BD noted: “[Children’s] homework diaries had the symptoms of depression… so we talked about it” (P05). A mother with BD used her academic assignments to educate her children: “I practised [a BD presentation] with my two kids… It was ‘Can you help me with my schoolwork?’, but also giving them that information at the same time” (P06).
Subtheme 4.3: ‘who should communicate’– family and professional supportInvolving other family members in sharing information about BD was seen by parents and professionals as important but challenging. Some participants preferred to explain the condition jointly with their partner. One father with BD shared: “We would have sat down together, my wife and I, and explained the whole thing” (P07). During crises, participants noted that “well” parents often took the lead in providing explanations, though they faced the urgency and difficulty of these situations. A father whose partner has BD described: “Suddenly it’s [mood episode] all happening, and I’m having to explain what is happening rather than being able to take my time explaining it in small chunks… before I’d been able to remove them [the children], they’d seen some really upsetting stuff, and I had to explain that in the context, it was really hard” (P10). How family members frame a BD episode can shape a child’s understanding and emotional response. A psychiatrist noted: “How they [children] react would depend on the people around them. If they have a sympathetic relative who explains that mummy is really unwell… versus somebody saying, ‘Oh, mummy was a bad person, she’s been taken away’… So it does depend on the extended family around them” (S12).
Professionals shared their experiences in assisting parents with BD to communicate their condition to their children, either by helping them prepare or guiding them during the conversation. One social worker explained: “[Helping parents] think through their fears… and have them heard and validated so that they can then do it for their children” (S09). Some professionals took the lead in communicating with children, similar to in psychoeducation sessions. A social worker described initiating these talks: “I can pop you [children] some appointments… let’s sit them down… What do you want to know, how can we make this open and inclusive?” (S10) Participants noted that professional involvement varied based on the child’s circumstances and the parents’ level of willingness. The social worker emphasised the need for flexibility: “Depending on… the age of the child, the demographics… the ability of the child to understand, and how much the parent is involved or wants you [the therapist] to be involved” (S10). She further stressed the importance of coordinating between adult and child mental health professionals: “There might already be a team around the child… let’s go into this [conversation] together… a trusted children’s colleague and me” (S10).
Comparative analysis of thematic contributionsWhile all subthemes incorporate perspectives from diverse roles, a comparative analysis of parents’ (parents with BD and non-bipolar partners) and stakeholders’ (professionals and charity workers) accounts highlights both shared and distinct perspectives on communicating about BD with children. Parents uniquely emphasised leveraging personal and familial experiences to tailor communication strategies, evident in their use of personalised language for age-adaptive communication (Subtheme 3.1), efforts to help children distinguish personality and typical behaviours from BD while reinforcing continuity (Subtheme 3.3), insights into future episode preparedness by avoiding overmedicalization, expressing emotional needs, and empowering children to help (Subtheme 3.4), and motivation driven by their own childhood experiences of non-transparent parental mental health communication to foster openness with their children (Subtheme 4.1). Among parents, non-bipolar partners did not tend to refer to communication advantages and challenges (Themes 1 and 2), likely prioritising practical strategies and support (Themes 3 and 4) due to their caregiving role for children and partners with BD. Conversely, stakeholders focused on the systemic and external factors that influence communication, highlighting the importance of support systems and social dynamics in addressing emotional and practical challenges, as exemplified in their recognition of honest dialogue to reduce children’s isolation (Subtheme 1.2), identification of complexities when both parent and child have mental health issues (Subtheme 2.1), acknowledgment of community stigma as a barrier (Subtheme 2.2), and emphasis on professional involvement, flexibility, and coordination in facilitating communication (Subtheme 4.3). However, most codes reflected the views of both groups, and the overall thematic structure were not dependent upon the small number of unique perspectives that were shared. This synthesis underscores the complementary nature of parents’ experiential insights and stakeholders’ systemic perspectives, enriching the thematic structure.
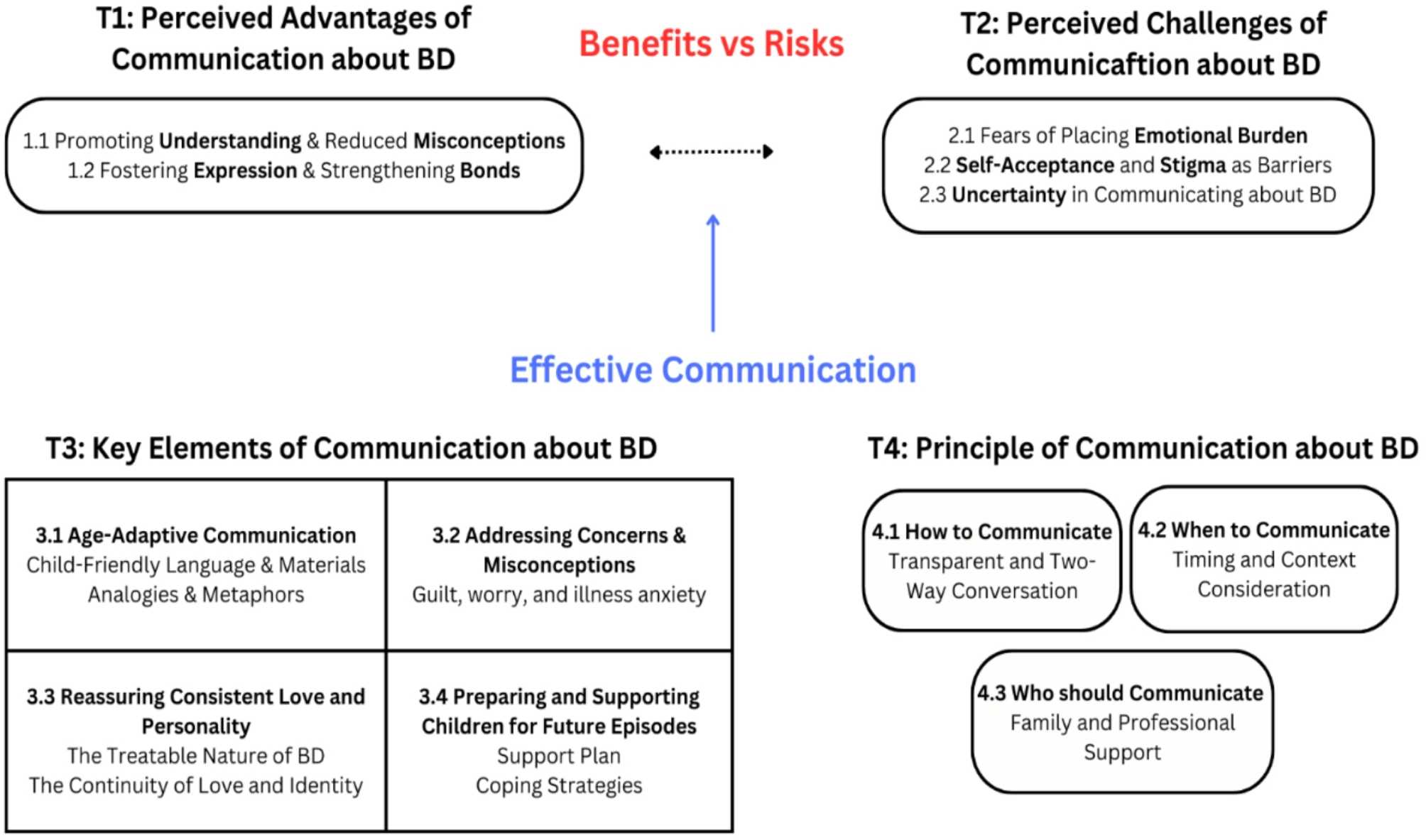
Fig. 1
The conceptual model depicting themes and sub-themes
Comments (0)