The history of Japanese immigration to Brazil is tied to the broader historical context of the Ryukyu Kingdom and Okinawa. The Ryukyu Kingdom, existed from 1429 until it was annexed by Japan in 1879, transforming into Okinawa Prefecture. Although became a part of Japan, it retained distinct cultural, linguistic, and historical differences 41, 42].
The formal relationship between Brazil and Japan was established in 1895 by the “Treaty of Friendship, Commerce and Navigation”, and in 1908, especially for the cultivation of coffee plantations after the abolition of slavery, the first wave of Japanese immigrants, including 325 Okinawans, arrived in São Paulo. In 1914, Okinawans settled in Campo Grande (MS), and by 1952, Brazil had become home to 229,000 Japanese immigrants [41, 42]. Despite confronted harsh conditions in coffee plantations in São Paulo and in the construction of the Noroeste do Brasil Railway, they made significant contributions to Brazil’s cultural and economic development [41, 42].
Currently, approximately 2 million Japanese descendants reside in Brazil, the largest community outside Japan, primarily concentrated in São Paulo (Southeast region), Mato Grosso do Sul (Central-West region), Paraná (South region), and Pará (North) states [30, 43]. Among the health challenges of in this population is an above-average incidence of people infected with the HTLV-1 virus. In Brazil, the first detection of HTLV-1 infection was identified among Japanese immigrants in Campo Grande, Mato Grosso do Sul, in 1986, with a prevalence of 10% [21]. Several studies conducted by our group among Japanese immigrants and their descendants found a high prevalence of HTLV-1 infection of 6.8% in Campo Grande, MS, and 5.1% in São Paulo [25, 26].
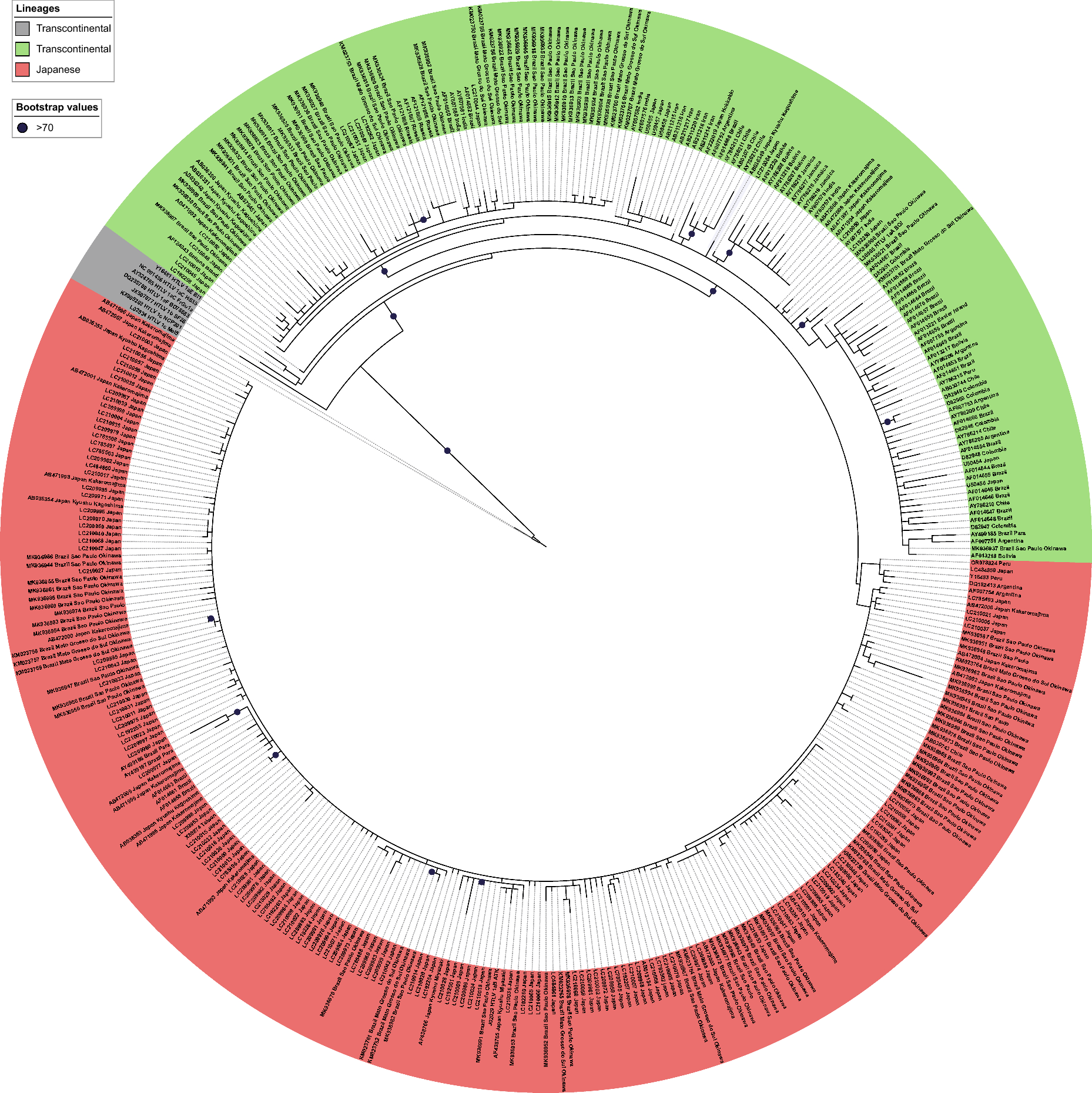
The HTLV-1 infection is endemic in some regions of Japan, and its distribution has a heterogeneous pattern, with a high prevalence in the Southwestern region, specifically in the Kyushu and Okinawa islands and in the North in Hokkaido, between indigenous population [4, 44]. The Transcontinental subgroup was initially introduced, followed by a second wave of migration introducing the Japanese subgroup [44]. Our data demonstrate that, after the introduction of these lineages into Brazil, the short period of time and the low mutation rate did not allow for the differentiation of specific clades. The Japanese and Transcontinental sequences obtained from our study, brought by Japanese immigrants to Brazil in the twentieth century, correspond to these prehistoric lineages from Japan.
A deeper look at the haplotypic variation patterns of the Japanese lineage revealed a typical star-like network (Fig. 4), where a central haplotype occurs in many individuals and is geographically widespread. This ancestral haplotype probably gave rise to several other minimally divergent haplotypes in a process of recent population expansion. The recent history of Japanese migration to Brazil [27] supports this finding. There has been insufficient time for the Japanese sequences from Japan and Brazil to differentiate, given the low evolutionary rate of HTLV-1.
The median-joining network and the time of divergence for the Japanese clade provide complementary information among the Japanese subgroup sequences, an interesting fact since the two analysis tools do not always generate congruent results [45]. The estimated time of divergence for the Japanese clade is approximately 18,000 years ago, and there is no geographical differentiation between the sequences from residents of Japan and the descendants of immigrants. The prehistoric origin of the lineage, combined with a low mutation rate and a recent population expansion, do not allow us to infer exactly which haplotypes came from Japan or when the exclusive haplotypes in Brazil emerged.
The current study represents the most extensive evolutionary analysis of HTLV-1aJpn infection in Brazil that has been conducted until now. However, some limitations must be acknowledged, such as the presence of a sampling bias, as the majority of the available sequences originated from Brazil and Japan may have influenced the study's findings. Furthermore, sequences accessible in GenBank were not included in our dataset due to the absence of geographic origin data, It is highly recommended that, during the inclusion of sequences in GenBank, researchers provide complete metadata to maximize the utility of available data in future studies. Furthermore, expanding future studies to include sequences from other South American countries with significant Japanese immigrant populations should be considered.
This study is the first in Brazil to extensively analyze the evolution of HTLV-1aJpn in the major Japanese population outside Japan. The presence of mixed viral sequences between Japanese and Brazilians, along with historical data, points to the recent migratory movements as responsible for the introduction of this lineage in Brazil. Given the significant prevalence of HTLV-1 within certain demographic groups, it is important to enhance epidemiological surveillance and implement screening strategies that consider historical and cultural factors. Essential actions include systematic HTLV-1 screening, coupled with culturally appropriate counseling and educational programs aimed at preventing sexual and intrafamilial transmission. These measures are crucial for improving public health policies and controlling HTLV-1 in diverse communities.






Comments (0)