
Remember me





Based on subtyping and phylogenetic analysis (Supplementary Fig. 1), a total of 245 individuals (141 treatment-naïve and 104 treatment-experienced) were classified as infected with CRF55_01B during the study period. Of these individuals, 236 (136 treatment-naïve and 100 treatment-experienced) full-length INT gene sequences were also successfully amplified. The age of them ranged from 17 to 76 years, with a median age of 36 years. 94.29% of them were men (231/245), and 44.08% of them were married. Among the main routes of infection, men who have sex with men (MSM) was the predominant transmission route (46.53%, 114/245), followed by heterosexual (HET) (31.84%, 78/245). Detailed characteristics of these CRF55_01B-infected individuals are shown in Table 1.
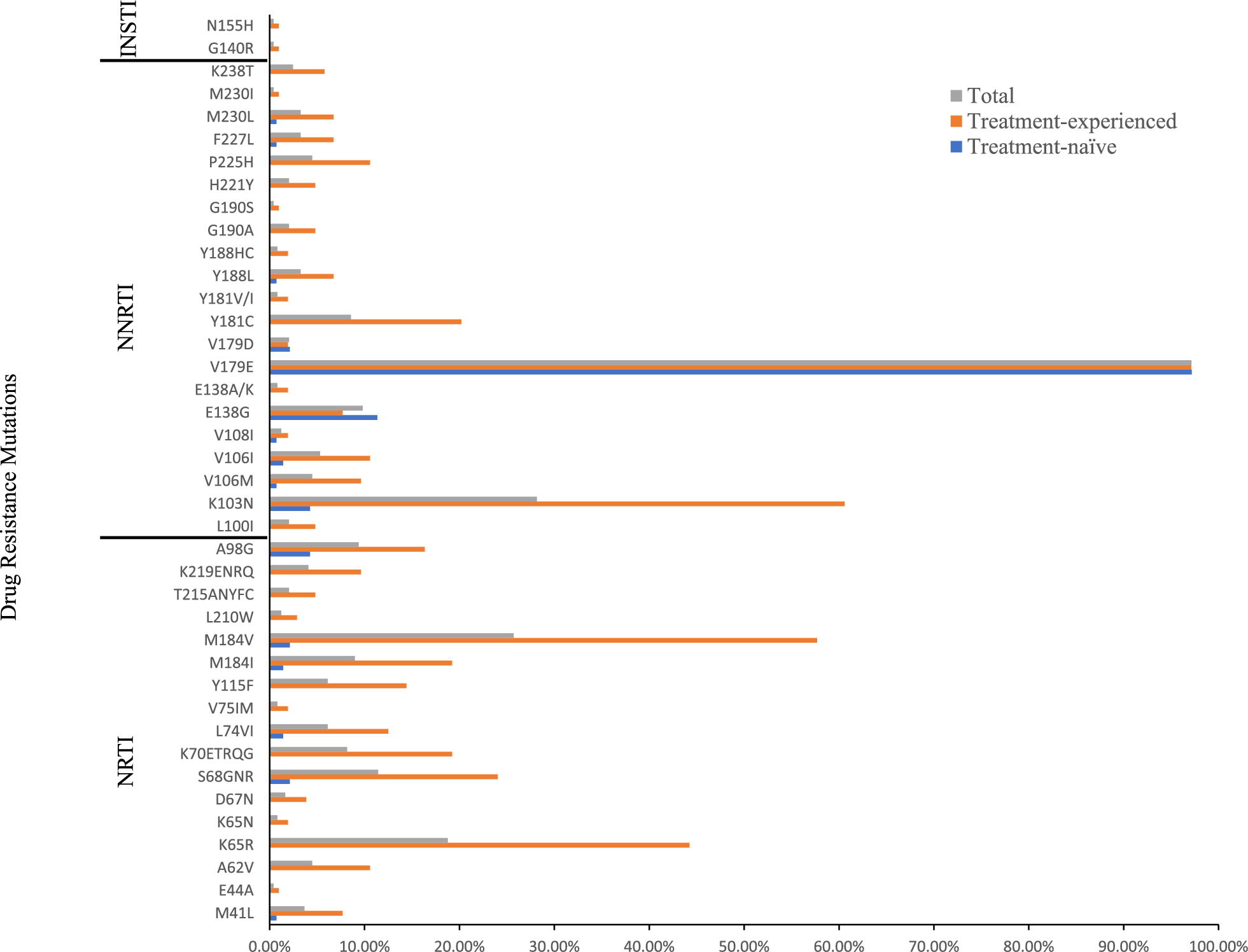
Table 1 Demographic characteristics of individuals infected with CRF55_01BPrevalence and distribution of DRMsOf the 245 CRF55_01B-infected individuals, 50.20% (123/245), namely, 21.28% (30/141) of the treatment-naïve individuals and 89.42% (93/104) of the treatment-experienced individuals, carried at least one DRM except V179E/D, which was present in all but two of them. In treatment-naïve individuals, 6.38% (9/141) of them harboured NRTI DRMs, 19.15% (27/141) of them harboured NNRTI DRMs, and none of them harboured PI and INSTI DRMs. Among the NRTI DRMs, M184V/I (3.55%, 5/141) was the most frequent, followed by S68G (2.13%, 3/141). Among the NNRTI DRMs, the most frequent mutation was E138G (11.35%, 16/141), followed by A98G (4.26%, 6/141) and K103N (4.26%, 6/141) (Fig. 1).
Fig. 1
The percentage of DRMs in the CRF55_01B-infected individuals in the treatment-naïve and treatment-experienced groups
In treatment-experienced individuals, 82.69% (86/104) of them harboured NRTI DRMs, 88.46% (92/104) of them harboured NNRTI DRMs, 2.00% of them (2/100) harboured INSTI DRMs, and none of them harboured PI DRMs. Among the NRTI DRMs, M184V/I (76.92%, 80/104) was the most frequent, followed by K65R (44.23%, 46/104), S68G/N/R (24.04%, 25/104), and K70 (19.23%, 20/104). Among the NNRTI DRMs, the most frequent mutation was K103N (60.58%, 63/104), followed by V106M/I (20.19%, 21/104), and Y181C (20.19%, 21/104) (Fig. 1). Dual-class mutations, namely NRTI plus NNRTI resistance mutations, were detected in 82.69% (86/104) of these individuals. The most common combination of mutations was M184V/I + K103N, with a frequency of 52.88% (55/104), followed by M184V/I + K65R, with a frequency of 39.42% (41/104). Triple-class mutations were found in one patient.
Drug resistanceAmong the 245 individuals, DRMs associated with low-level or higher levels resistance to any drug was detected in 49.39% (121/245): NRTIs (37.55%, 92/245), NNRTIs (48.57%, 119/245) and INSTIs (0.85%, 2/236). The prevalence of pretreatment drug resistance (PDR) was 19.86% (28/141), while the overall prevalence of acquired drug resistance (ADR) was 89.42% (93/104). In treatment-naïve individuals, drug resistance to NRTIs and NNRTIs accounted for 4.26% (6/141) and 19.15% (27/141), respectively, and drug resistance to PIs and INSTIs were not detected. In treatment-experienced individuals, drug resistance to NRTIs, NNRTIs, and INSTIs accounted for 82.69% (86/104), 88.46% (92/104), and 2.00% (2/100), respectively, and resistance to PIs was not detected (Fig. 2).
Fig. 2
The percentage of drug resistance in the CRF55_01B-infected individuals in the treatment-naïve and treatment-experienced groups
Resistance to commonly used drugs in clinical settings was further analyzed. Intermediate- to high-level resistance to lamivudine (3TC) and emtricitabine (FTC) of the NRTIs was the most prevalent in treatment-experienced individuals, followed by abacavir (ABC), and the same pattern was observed in treatment-naïve individuals. For NNRTIs, intermediate- to high-level resistance to nevirapine (NVP) was the most commonly observed in both treatment-experienced and treatment-naive individuals, followed by efavirenz (EFV) and rilpivirine (RPV). For INSTIs, resistance to cabotegravir (CAB), raltegravir (RAL), and elvitegravir (EVG) was observed in treatment-experienced individuals (Fig. 3).
Fig. 3
Different drug resistance levels of four classes of antiretroviral drugs predicted by the Stanford HIVdb Program the CRF55_01B-infected individuals in the treatment-naïve and treatment-experienced groups. ABC abacavir, AZT zidovudine, FTC emtricitabine, 3TC lamivudine, TDF tenofovir, DOR doravirine, EFV efavirenz, ETR etravirine, NVP nevirapine, RPV rilpivirine, DRV/r darunavir/r, LPV/r lopinavir/r, BIC bictegravir, CAB cabotegravir, DTG dolutegravir, EVG elvitegravir, RAL raltegravir
Transmission characteristicsConsidering the high-level of PDR and ADR in CRF55_01B-infected individuals, we further performed molecular network analysis to determine if individuals with PDR could be traced to individuals with ADR. Under the threshold of 1.5% genetic distance, sequences from both treatment-naïve and treatment-experienced individuals formed a total of 23 transmission clusters (TCs), accounting for 37.55% (92/245) of the total sequences. These TCs ranged in size from 2 to 19, and 15 (65.22%) had 3 or more sequences. Drug resistance was identified in 13 TCs and 7 of these TCs (47 sequences) contained both treatment-naïve and treatment-experienced individuals (Fig. 4).
Fig. 4
The transmission networks of CRF55_01B-infected individuals. Different colors are used to represent treatment-naïve and treatment-experienced, respectively. Rectangle represents drug resistance
Comments (0)