Obesity is a well-established risk factor for EMC, and many studies have revealed that the average BMI of patients undergoing surgery for EMC exceeds 30 [10, 13,14,15,16,17, 19,20,21,22,23,24,25,26]. According to 2017–2018 data from the National Health and Nutrition Examination Survey, 27.5% of American women are overweight (BMI 25–29), and 41.9% are obese (BMI > 30) [27]. In contrast, the average BMI of Japanese women is approximately 22, and 22.3% have a BMI > 25, with no significant change over the past two decades.
Reports from Japan show that the average BMI of EMC patients ranges from 23 to 26 [28, 29], similar to other East Asian populations [30, 31].
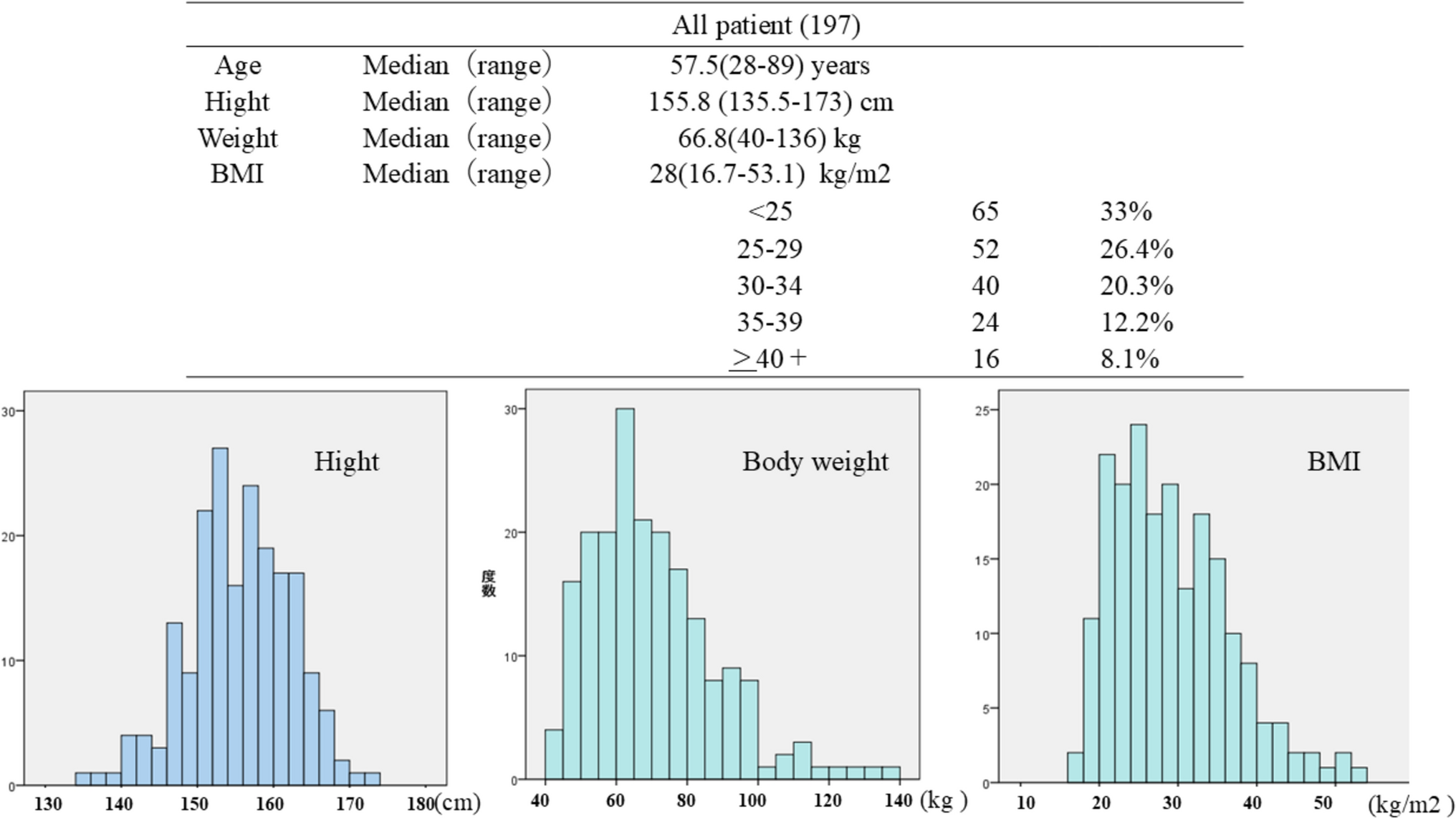
In EMC patients, HT is reported in more than 50% of those with a BMI > 30 and 58–74% of those with a BMI > 40, although significant differences according to obesity category are often not observed [13, 20, 26, 32, 33]. In contrast, the prevalence of DM varies across studies depending on BMI, ranging from 21.6% to 39.5% for individuals with a BMI > 30 [13, 20, 26, 32, 33]. In this study, the prevalence of DM was 51.3% in individuals with a BMI > 30, similar to Japanese data revealing a prevalence of 46% in individuals with a BMI 30–39 [21]. While the prevalence of DM is typically reported to be 7–18% in individuals with a BMI < 30 [21, 26, 34, 35], our data revealed a higher prevalence of 35.8%, even in patients with a BMI ranging from 25–29. These findings suggest that Japanese patients tend to have a higher prevalence of DM than other populations do, especially if they have a BMI > 25.
Obesity is generally associated with worse surgical outcomes, and the incidence of complications tends to increase with increasing BMI [36]. However, many reports have revealed that RA, as a minimally invasive surgery, is associated with a lower incidence of complications than conventional laparotomy is and can be performed safely and effectively in obese patients [5, 12, 16, 17, 23, 24, 36, 37], but the operation time is longer than that of conventional laparotomy [12, 23, 38]. In our hospital, the operative time tended to be shorter for minimally invasive procedures than for open surgery, possibly due to a high level of surgical experience and reduced closure times in obese patients (data not shown). Many studies have revealed that there are no significant differences in operative outcomes or perioperative complication rates of RA, regardless of BMI [11, 13, 19, 20, 26, 33]. Our data similarly revealed differences between obese patients (BMI > 30) and those with a BMI < 30. Moreover, some have noted that the incidence of complications increase with increasing BMI [37], as evidenced by a higher incidence of wound infections in patients with a BMI > 40 [13]. Similarly, our data revealed a significantly higher rate of Class II postoperative pelvic infections in patients with a BMI > 35.
Survival outcomes for EMC are generally favorable, with many reports indicating no significant differences between laparotomy and laparoscopic surgery [14, 15, 25]. In addition, a prospective study conducted in Australia investigated the long-term prognosis of 760 obese cancer patients who underwent laparotomy or laparoscopic surgery, with approximately 60% having a BMI of 30 or more and a follow-up period of 4.5 years [24]. The study revealed no difference in recurrence rates, which were approximately 8%. Across all the cases, new cancers were observed in approximately 8.4% of patients, with 3.9% of deaths attributed to EMC and 3.1% attributed to other causes. Similarly, our data revealed a relatively favorable survival outcome for EMC, with a mortality rate of 1% during a median follow-up period of 3 years. However, research suggested that new cancers, as well as obesity- and diabetes-related conditions such as cardiovascular disease and renal failure, may impact long-term survival outcomes.
In terms of costs, while robotic surgery is highly effective, many reports highlight its higher cost compared to laparotomy and laparoscopic surgery, raising concerns about the financial burden on healthcare systems [12, 17, 19, 23, 39, 40]. On the other hand, studies have revealed that higher annual surgical volumes could improve cost-effectiveness [12], and robotic surgery in patients aged 70 and older has been reported to provide overall good cost-performance [35]. Our healthcare cost data revealed that both the actual billed amount and surgical costs were significantly higher for patients with a BMI ≥ 30. As previously mentioned, the difference between the costs billed under the DPC system (actual billed amounts) and those recalculated under the FFS system (reference values) was greater in patients with a BMI ≥ 30 than in those with a BMI < 30. This is likely due to an increase in non-billable medical procedures under the DPC system, such as the additional use of medications, intravenous fluids, and interventions required for higher body weight and comorbidities. These findings suggest that patients with a BMI ≥ 30 may impose a greater financial burden not only on themselves but also on hospitals and national healthcare resources. Furthermore, we speculate that non-quantifiable factors—such as the increased workload for healthcare staff related to patient transfer and repositioning—may also contribute to the overall cost.
In this study, robotic surgery was performed safely across BMI categories, suggesting that obesity alone may not adversely impact surgical safety in a well-managed perioperative setting. This raises the question: Is preoperative weight loss truly necessary? While our data did not show a direct link between weight reduction and surgical outcomes, previous studies have demonstrated that morbid obesity (BMI > 40) is associated with an increased risk of perioperative complications. Additionally, anesthesiologists and gynecologic surgeons may experience greater psychological and physical stress when managing severely obese patients in the steep Trendelenburg position. As noted earlier, preoperative weight loss may help reduce the use of medical resources, prevent the progression of obesity-related comorbidities, and lessen the physical burden on healthcare personnel. Therefore, we believe that preoperative weight management remains an important element of comprehensive perioperative care in patients with obesity.
At the same time, while this study does not propose specific policy recommendations, our findings suggest that investing in public health efforts to prevent obesity and lifestyle-related diseases may ultimately be more cost-effective than focusing solely on the treatment of complications using advanced medical technologies. In light of these findings, we believe that future healthcare policies should consider balancing investments in high-cost treatments with broader public health initiatives aimed at preventing obesity and improving population health.
The limitations of this study include its retrospective design, use of single-institution data, and its relatively small sample of cases. Healthcare costs cannot be definitively assessed only on the basis of these data, and larger studies are needed. However, with an average height of 155.3 cm and a high proportion of obese patients, our findings offer valuable insights into the outcomes and cost of robotic surgery for obese EMC patients, particularly in Japanese and Asian populations.

Comments (0)