
Remember me
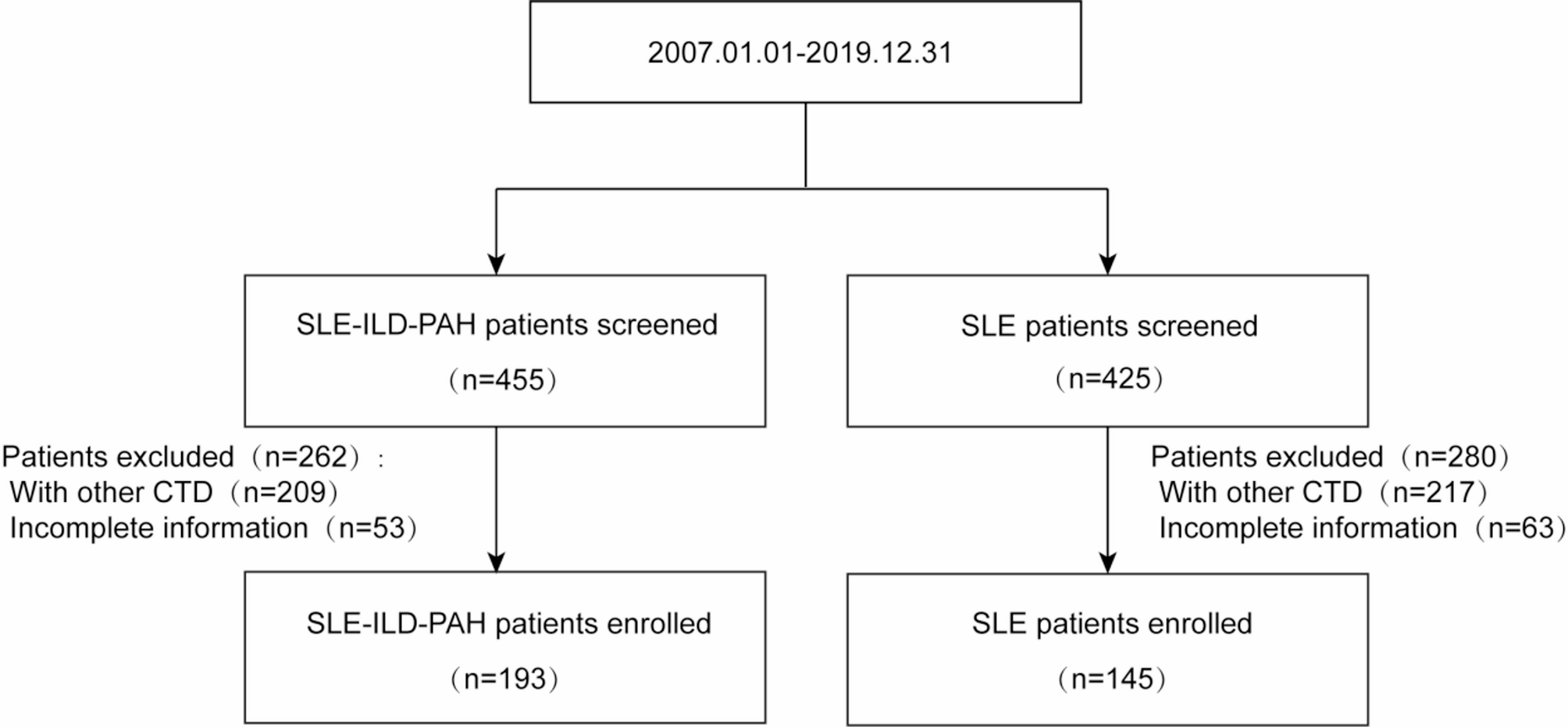

From an initial cohort of 880 patients with SLE, we excluded 426 patients with overlapping CTDs and 116 patients with incomplete clinical data. The final study population comprised 338 SLE patients (median age: 40.37 years; 93.2% female), consistent with epidemiological data highlighting female predominance in SLE and its associated pulmonary complications [14].
Among these, 193 patients (57.1%) were diagnosed with both ILD and PAH based on pulmonary HRCT scans and TTE, while 145 served as non-ILD/PAH controls. Baseline characteristics are detailed in Table 1.
Compared to SLE-only patients, the SLE-ILD-PAH group exhibited: significantly higher inflammatory markers: elevated CRP, ESR, neutrophil percentage, and neutrophil-to-lymphocyte ratio (NLR); more severe disease activity: higher SLEDAI scores; distinct clinical features: older age, higher prevalence of pleuritis, pericarditis, fever, and thrombocytopenia; laboratory abnormalities: lower hemoglobin, erythrocyte counts, lymphocyte counts, lymphocyte percentage, and anti-dsDNA titers (all p < 0.01). No differences were observed in height, weight, SLE duration, neutrophil counts, monocyte counts, monocyte percentage, hypocomplement, or leukopenia (all p > 0.05).
Table 1 Clinical characteristics of the participantsScreening strategies for PAH in SLECurrent guidelines from the European Society of Cardiology/European Respiratory Society (ESC/ERS) and the American College of Cardiology Foundation/American Heart Association (ACCF/AHA) emphasize TTE as the primary screening tool for PAH, given its non-invasive nature and ability to estimate pulmonary artery pressure [18,19,20]. While right heart catheterization (RHC) remains the diagnostic gold standard, its cost and invasiveness limit widespread use. In clinical practice, a peak tricuspid regurgitation velocity (TRV) > 2.8 m/s on TTE is a well-validated risk marker for SLE-PAH [21]. Our screening protocol aligned with these recommendations, tailored to regional resource availability. Table 2 lists TTE characteristics of SLE-ILD-PAH patients in our cohort.
Table 2 TTE characteristics of SLE-ILD-PAH patientsSelection of predictor variablesAll of the variables were coded as binary based on their average levels in SLE and SLE-ILD-PAH groups (seen in Table 1). Univariate logistic regression identified 24 variables associated with SLE-ILD-PAH (Table 3). Odds ratios and 95% confidence intervals (CI) were estimated by fitting the logistic proportional hazards models. Age, gender, CRP, ESR, hemoglobin, neutrophil, neutrophil%, lymphocyte, lymphocyte%, neutrophil/lymphocyte, pleuritis, pericarditis, anti-dsDNA, fever, thrombocytopenia, leukopenia, and SLE Disease Activity Index (SLEDAI) were selected into subsequent multivariate logistic regression analysis. Five variables were selected for independent predictors: positive associations: age (OR: 2.534, 95% CI: 1.317–4.877), CRP (OR: 3.963, 95% CI: 1.941–8.092), pericarditis (OR: 9.769, 95% CI: 4.965–19.221), and SLEDAI (OR: 2.161, 95% CI: 1.102–4.239); negative association: anti-dsDNA positivity (OR: 0.400, 95% CI: 0.212–0.755).
To evaluate potential information loss, we repeated univariate logistic analyses using continuous variables (age and others), confirming that our findings remain materially unchanged (Supplemental Table S1), except for the differences in the analysis results of erythrocyte between continuous variables and categorical variables, which does not affect the final model construction.
Table 3 Logistic analysis of predictive factors for SLE-ILD-PAH (n = 338)Construction and evaluation of SLE-ILD-PAH diagnostic nomogram modelAge, CRP, pericarditis, anti-dsDNA, and SLEDAI were used to develop the prediction model. This prediction algorithm is graphically summarized as a nomogram in Fig. 2A. To demonstrate how the nomogram works, we provided a detailed clinical example that walks through the scoring process visually. Consider a 58-year-old SLE patient, they score 38 points for their age, 30 points for having a negative anti-dsDNA antibody, 21 points for an SLEDAI of 16, 21 points for a CRP level of 8, 8 points for the absence of pericarditis. Adding these up, the total score is 118 points, which corresponds to a 62.9% risk of ILD-PAH. This step-by-step breakdown shows how the nomogram can be used to assess risk in a clear and visual manner. The predictive ability of the nomogram model was evaluated using the calibration curve, and as shown, the nomogram model had high accuracy in predicting SLE-ILD-PAH (Fig. 2B). Meanwhile, the DCA showed that the nomogram curve was above the blue line, indicating that patients could benefit from the nomogram model (Fig. 2C). Table 4 listed sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), AUC, p-value and 95% CI of five variables and the combined variable in ROC analysis. Combined all the 5 variables significantly improved the predictive performance (AUC = 0.871, 95% CI: 0.833–0.910), demonstrated excellent discrimination (Fig. 3A-B). Finally, forest plot analysis further confirmed the diagnostic weight of each variable (Fig. 3C).
Fig. 2
Nomogram performance. A, Nomogram predicting SLE-ILD-PAH. B, Calibration curve of the nomogram. C, DCA of the nomogram
Table 4 ROC analysis of predictive variables for SLE-ILD-PAHFig. 3
Discrimination validation of the nomogram model. A-B, ROC analysis. C, Forest plot analysis
Comments (0)