
Remember me

In our research project, we follow the framework for developing and evaluating complex health interventions by the UK Medical Research Council [22]. This framework aims to support the implementation of interventions that are not only effective but also “acceptable, implementable, cost-effective, scalable, and transferable across contexts” (p. 2 [22]). It outlines four key steps: (1) identifying or developing a potentially suitable and beneficial intervention, (2) testing its feasibility, (3) evaluating its effectiveness, and (4) facilitating its implementation. Based on findings from a previous study that identified the need for and potential of a digital MBI for individuals with COPD [20], we developed the intervention examined in this pilot study (step 1). The current pilot randomised controlled trial corresponds to step 2 of the framework. Its objective was to assess the feasibility of an 8-week self-administered digital MBI to identify potential challenges and adaptation criteria for a future large-scale randomized controlled trial (step 3), and to gather preliminary data on the intervention’s effects to inform power calculations and determine which observed trends may be promising for further investigation in a future definitive trial (based on recommendations for pilot studies [22,23,24]).
The primary outcome was feasibility among individuals with COPD and elevated levels of anxiety or depression by examining (a) dropout rates, (b) usage behaviour, (c) patients’ experiences as reported in telephone interviews after 8 weeks, and (d) long-term treatment adherence after 6 months. Further, we aimed to assess the intervention’s preliminary effects and hypothesised that the MBI may reduce levels of anxiety and depression after 8 weeks. Regarding secondary outcomes, we hypothesised reduced self-reported stress, lower physical health impairment, and improved COPD-related quality of life in the intervention group after 8 weeks. We further investigated basal activity and stress reactivity of two bodily stress systems (ANS and HPA axis) to explore possible changes in these systems’ functioning due to the MBI. We therefore hypothesized lower hair cortisol levels (correlate of basal HPA axis activity reflecting cumulative cortisol secretion over several months [7]), and improved stress reactivity on a subjective and biological level (assessing heart rate, heart rate variability, and skin conductance level as correlates of ANS reactivity [7]) in the intervention group after 8 weeks. Finally, we investigated momentary subjective stress, anxiety, and dyspnoea immediately before and after the individual MBI activities from an exploratory perspective.
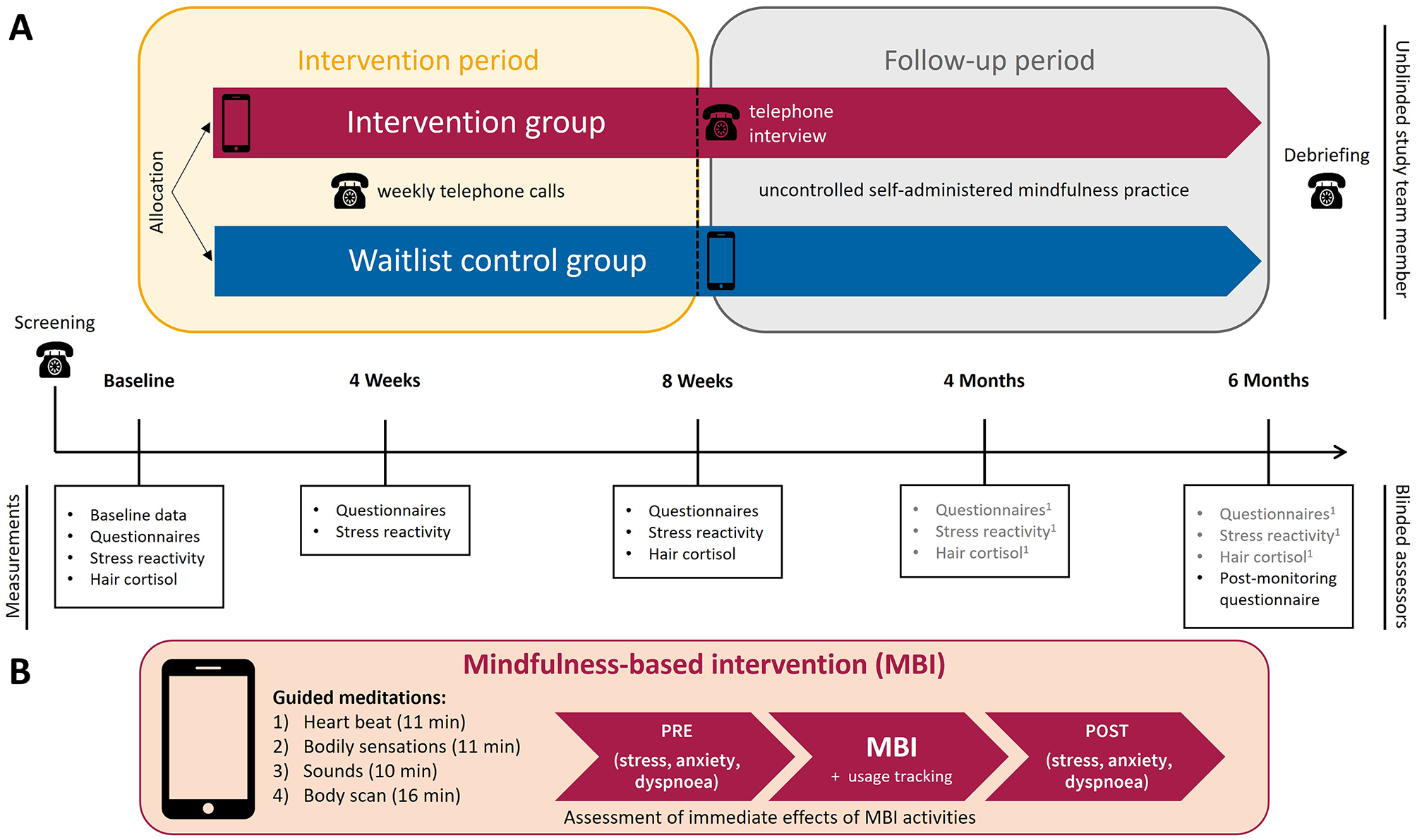
An overview of the study is provided in Fig. 1. The study was in accordance with the Declaration of Helsinki, approved by the city of Vienna ethics review board (serial number: EK 20–177 VK), and preregistered at ClinicalTrials.gov (identifier: NCT04769505).
Fig. 1
Study overview. Note.(A) Study timeline. Measurements were conducted in patients’ homes (see Suppl. 1 for COVID-19 protocol to ensure safe in-person contact) to include non-mobile patients, unless patients explicitly preferred assessments in the laboratory at the University of Vienna. 1These data are not relevant to the scope of this publication. (B) Mindfulness-based intervention (MBI). Icons provided by www.flaticon.com
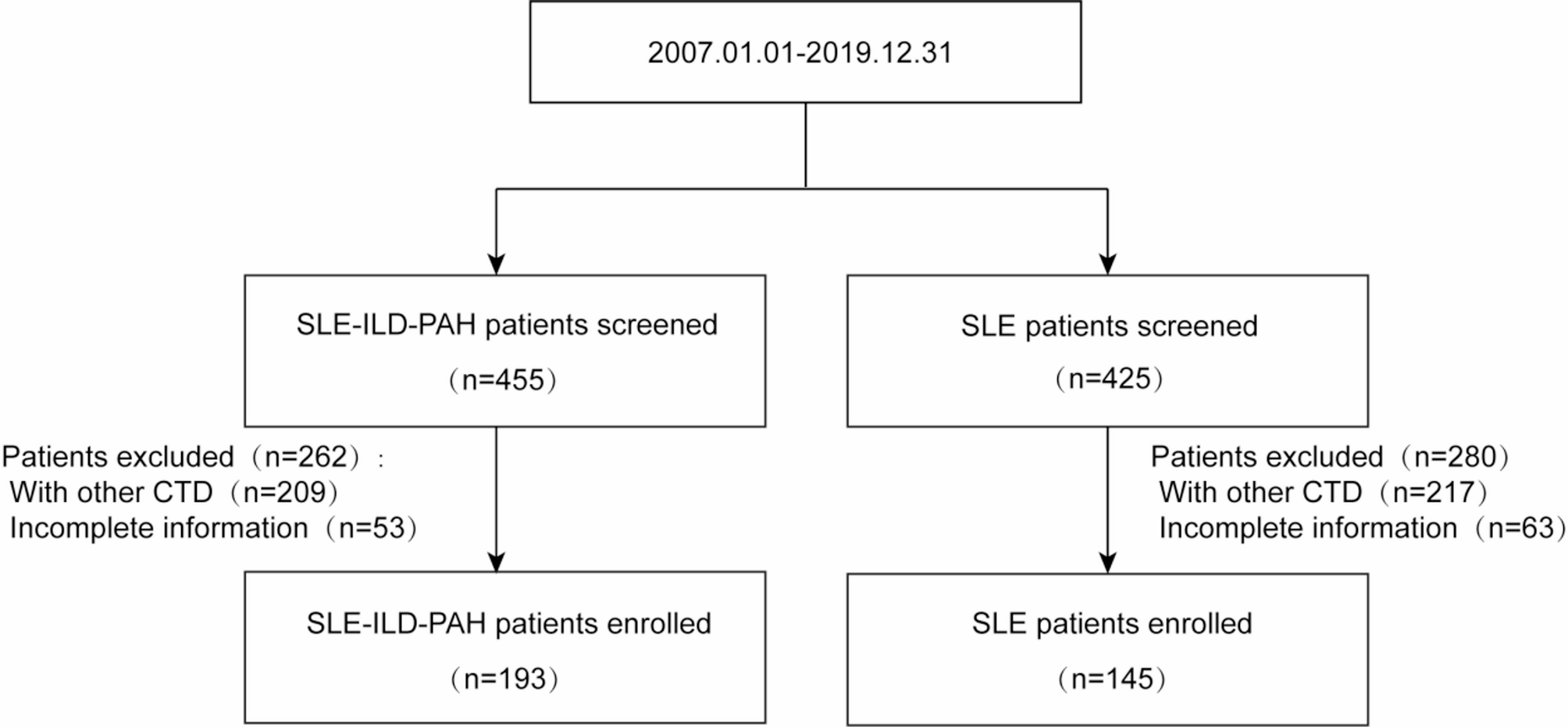
ParticipantsWe aimed to recruit 30 COPD patients (n = 15 per treatment arm) completing the intervention period, based on the sample size recommendations for pilot studies aiming at a 90%-powered main trial [24], assuming a medium effect size (0.3 ≤ d ≤ 0.7) for symptoms of anxiety, depression, and stress for an 8-week intervention effect [15]. According to the CONSORT extension to pilot studies, the sample size should be determined based on the feasibility objective [23]. Our sample size is adequate to determine feasibility, consistent with studies using similar methods (e.g. sample range of 5–32 for qualitative meta-synthesis by [13]). Outpatients with stable COPD from two clinics and a rehabilitation centre were contacted for screening (see Fig. 2 for details on recruitment and study flow). Eligible patients (see Table 1 for eligibility criteria) received detailed information about study participation and provided written informed consent at baseline. Baseline participant characteristics are summarised in Table 2 (for full baseline characteristics, see Table S1).
Fig. 2
Study flow and recruitment diagram. Note. Following the study preparation phase (September 2020 – March 2021), patients were recruited from March 2021 – December 2022, until 30 participants concluded the intervention period. Assessments lasted from March 2021 – March 2023
Table 1 Inclusion and exclusion criteriaTable 2 Selected baseline characteristicsRandomisation and blindingFollowing a baseline session, patients were randomised to the intervention (MBI plus treatment as usual (TAU)) or waitlist control group (TAU) using block randomisation (allocation ratio 1:1; random block lengths of 2, 4, and 6), stratified by patients from the respiratory unit Floridsdorf on a waitlist for a bronchoscopic lung volume reduction (as these had been preselected regarding their eligibility for the procedure) and all other patients. The random treatment allocation was generated for each sub-sample by one study team member prior to data collection. After baseline, the same study team member informed the patient by telephone about the treatment allocation. The assessors conducting the recruitment and measurements were blinded regarding treatment allocation. The assessor blinding was broken during 26 measurements (23%), as patients articulated their treatment allocation.
TreatmentThe four auditory-guided meditations (for details see Fig. 1) are based on mindfulness-based cognitive therapy [26] and its adaptations for COPD patients (e.g., heartbeat as an anchor) by Farver-Vestergaard and colleagues [27] and were further adapted for this study (e.g., shortened, simpler language). The audios were delivered via the movisensXS software (Movisens GmbH) installed on patients’ (study) smartphones. Patients received an individual face-to-face introductory session (30–50 min) and were instructed to practice at least once daily during the intervention period. Additionally, an intervention manual (Supplementary Material 2 at https://osf.io/sx5h9/) and a weekly telephone call supported their self-administered mindfulness practice. After 8 weeks, the intervention group received the MBI meditations as audio files with the instruction to continue practicing in the follow-up period.
Waitlist patients received the MBI after the intervention period, with the same instructions, manual, and introductory session as the intervention group. However, the meditations were provided directly as audio files. To control for the psychological support provided by the weekly telephone calls, the study team also called the waitlist group weekly during the intervention period to discuss health status and experiences of the past week.
MeasuresPrimary outcomesTo assess feasibility, the dropout rate was defined as the number of patients who started the study but dropped out before concluding the intervention period. Usage behaviour was defined as the number of meditations (≥ 10 min) conducted by the intervention group within the intervention period, using log numbers from the study software. The telephone interviews with intervention group participants after 8 weeks assessed the acceptability and usability of the intervention and participants’ satisfaction using and open-ended entry question, closed questions, and open-ended follow-up questions (for details see Suppl. 3 and Supplementary Material 1 at https://osf.io/sx5h9/). Interviews were conducted by one study team member and were audiotaped. The structured post-monitoring questionnaire assessed long-term adherence to the self-administered mindfulness practice in the follow-up period using three dichotomous items (“Did you conduct mindfulness activities during the last 4 months?”, “Did you use the study mindfulness activities during the last 4 months?”, “During the past 4 months, have you performed other mind-body techniques such as relaxation exercises, meditation, autogenic training, imaginative processes, yoga, qi gong, or tai chi?”, for details see Suppl. 4).
Symptoms of anxiety and depression were assessed at three measurement time points (baseline, 4 weeks, 8 weeks) using the corresponding subscales and sum score of the Hospital Anxiety and Depression Scale (HADS) [25]. Sum scores for each scale range from 0 to 21, with higher scores representing higher symptom burden (Anxiety, HADS-A: α = 0.71, Depression, HADS-D: α = 0.80).
Secondary outcomesThe Perceived Stress Scale (PSS-10) [28] was used to assess self-reported ongoing stress at three measurement time points (baseline, 4 weeks, 8 weeks). Sum scores range from 0 to 40, with higher scores indicating higher stress (α = 0.82). Physical health impairment was assessed at three measurement time points (baseline, 4 weeks, 8 weeks) using the COPD Assessment Test (CAT) [29]; sum scores range from 0 to 40, with higher scores indicating greater impairment (α = 0.80). COPD-related quality of life was assessed at three measurement time points (baseline, 4 weeks, 8 weeks) using the Chronic Respiratory Questionnaire Self-Administered Standardized (CRQ-SAS)Footnote 1 [30], with items rated from 1 to 7, covering four domains: dyspnoea (α = 0.85), fatigue (α = 0.81), emotional function (α = 0.80), and mastery (α = 0.73).
Hair samples were collected at two measurement time points (baseline, 8 weeks) to analyse cumulative hair cortisol concentration (pg/mg) from the last two months (2-cm segments of scalp-near hair). Analyses were conducted by the biochemical laboratory at the Faculty of Psychology, University of Vienna, following the analysis protocol by Stalder and colleagues [31].
Stress reactivity was measured at three measurement time points (baseline, 4 weeks, 8 weeks) during a stress induction protocol using a cognitive stressor (modified Stroop task, based on [32, 33], adapted for this study; for details see Suppl. 2 including Figure S1). Momentary subjective stress was assessed at five time points (5 min before Stroop, before Stroop, after Stroop, 5 min after Stroop, 10 min after Stroop) during the stress induction protocol, using a unipolar visual analogue scale (“At the moment I feel stressed”) ranging from 0 (not at all) to 100 (very much). Stress-related ANS reactivity markers (heart rate (HR), root mean square of successive difference (RMSSD) indicating heart rate variability, and skin conductance level, SCL) were continuously measured during the stress induction protocol, using Movisens sensors (Movisens GmbH). Stress reactivity was calculated as the difference score between the time point 5 min before and right after the Stroop task for momentary subjective stress, and between the 5 min before and the Stroop task interval for ANS markers (HR, RMSSD, SCL), ensuring that all measures reflect the change from the initial resting state to peak stress exposure. Details regarding biomarker assessments are described in Suppl. 5.
Exploratory outcomesTo assess the immediate effects of meditation, patients reported their momentary subjective stress, anxiety, and dyspnoea via the study software before and after each meditation in the intervention period. Momentary subjective stress was assessed on a visual analogue scale (item description in the previous paragraph). Anxiety was assessed using an adapted HADS item (“I feel anxious”) with four response options ranging from 0 (not at all) to 3 (very). Dyspnoea was measured using a modified Borg Scale [34] with twelve response options ranging from 0 (no breathlessness at all) to 10 (maximal breathlessness).
Data analysisDescriptive statistics were calculated using Excel (Microsoft 365) and IBM SPSS (Version 28.0.1.1). Telephone interviews were fully transcribed semantically by a project assistant. The answers to the closed interview questions were noted by the interviewer and verified using the transcripts. Answers to the open-ended questions were qualitatively analysed by the interviewer following the steps of reflexive thematic analysis (software: MAXQDA Plus, Version 22.2.0) [35]. Primary and secondary analyses comparing groups over time were analysed using linear mixed models. This deviates from our preregistered analysis using repeated measures ANOVAs, as linear mixed models are the recommended state-of-the-art analysis approach for our data structure [36]. We specified two-level models (measurements nested within participants), with the factors time (baseline, 4 weeks, 8 weeks), group (intervention, waitlist), and crossed factors time x group (intervention effect), using restricted maximum likelihood estimation and the Kenward-Roger approximation. Outliers were not excluded from the analysis, with the exception of eight RMSSD outliers that were due to technical issues. Number of medications was added to the models assessing biological outcomes as a level-2 grand-mean centred covariate [37]. Exploratory analyses were conducted using a two-level linear mixed model with the factor time (pre, post meditation), restricted maximum likelihood estimation and the Kenward-Roger approximation. Effect sizes were described as partial eta-squared (ηp2) calculated from F-tests. All linear mixed models were calculated in R (Version 4.3.0). Details on data analysis and data preprocessing of the biodata are described in Suppl. 6. Sensitivity analyses (removing outliers, including/removing covariates, calculating a robust model with the R package robustlmm [38]) were conducted to gain additional insights into the data (see Suppl. 7). However, given the small sample size, all results regarding intervention effects should be considered preliminary.
Comments (0)