
Remember me


Between 2018 and 2022, 24 patients with type II or type III SMA received posterior spinal fusion for scoliosis at our center. Patient demographics are summarized in Table 1. Individual patient data is available in Supplementary Table 5. Of these patients, 14 were females and 10 were males, ranging in age from 10 to 28. There were 16 patients with SMA type II and 8 patients with SMA type III.
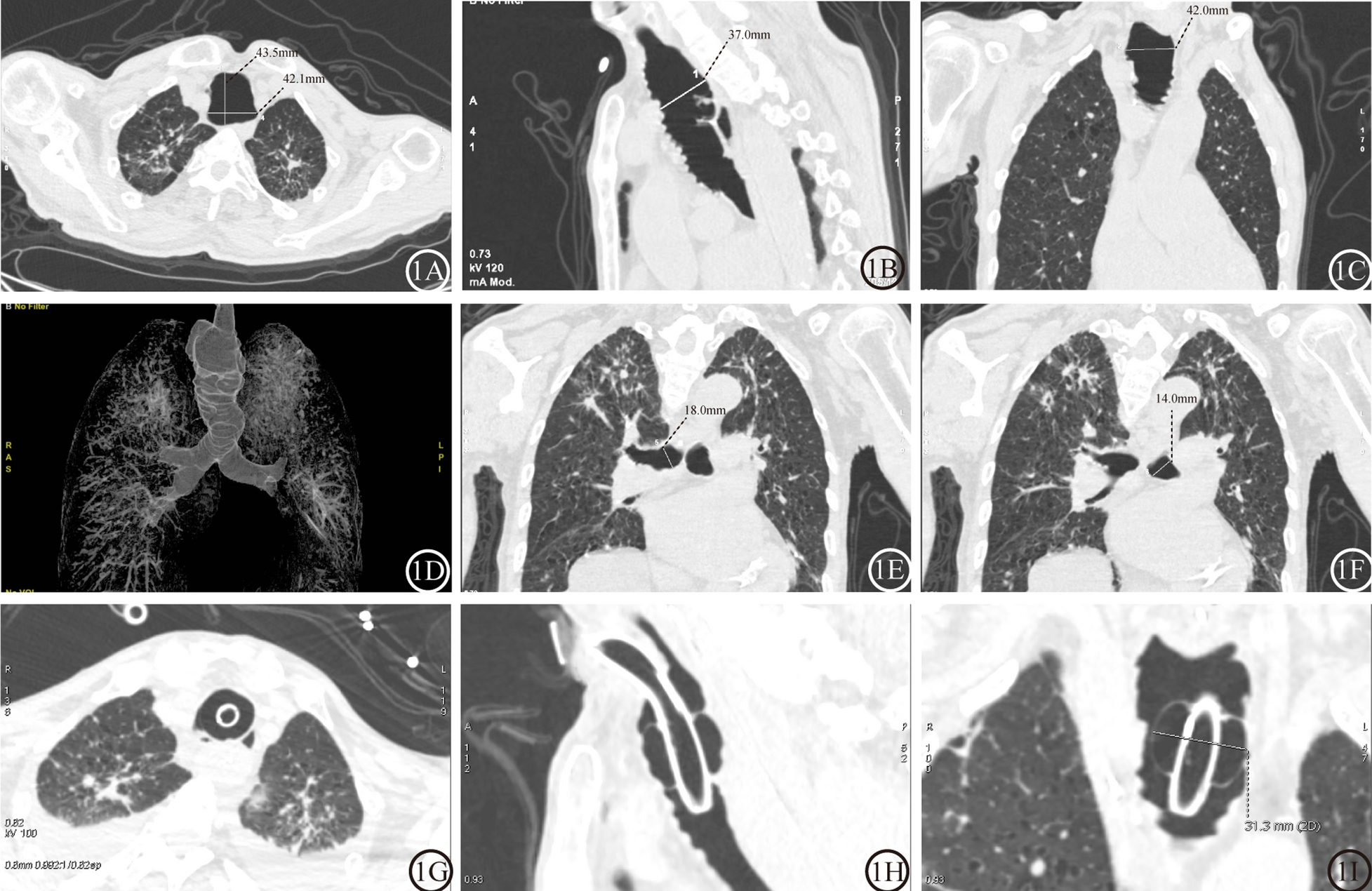
Table 1 Patient demographics and clinical characteristicsClinical characteristicsAll patients (24/24) had severe scoliosis, kyphosis, or kyphoscoliosis, with a mean Cobb angle of 102 degrees. All patients (24/24) had prominent muscle weakness. For the pulmonary function test, three patients were physically unable to complete it due to severe respiratory impairment and were therefore classified as having severe respiratory impairment. Consequently, pulmonary function tests revealed that 95.8% of the patients (23/24) exhibited impaired pulmonary function, among which 58.3% of the patients (14/24) had severely impaired pulmonary function. Airway stenosis including tracheal deviation, recurrent airway infections including recurrent pneumonia, and/or asthma was observed in 37.5% of the patients (9/24). Overnight ventilatory support was required in 12.5% of the patients (3/24). All patients (24/24) were classified as total or severe dependency according to the Barthel Index, and all (24/24) were at risk of developing pressure sores as predicted by the Braden Scale. NRS 2002 scores were available for 22 patients, among whom 54.5% (12/22) were at nutritional risk. Nutritional states could not be assessed in two patients since they were not able to leave the bed due to severe spinal curvature or muscle weakness. All patients received posterior spinal fusion with bone grafting, and only one patient developed a major postoperative complication, pneumonia, which was effectively managed. Anxiety level decreased significantly (P = 5.983 × 10−14) at discharge compared to that on admission. Detailed clinical characteristics are available in Supplementary Table 5.
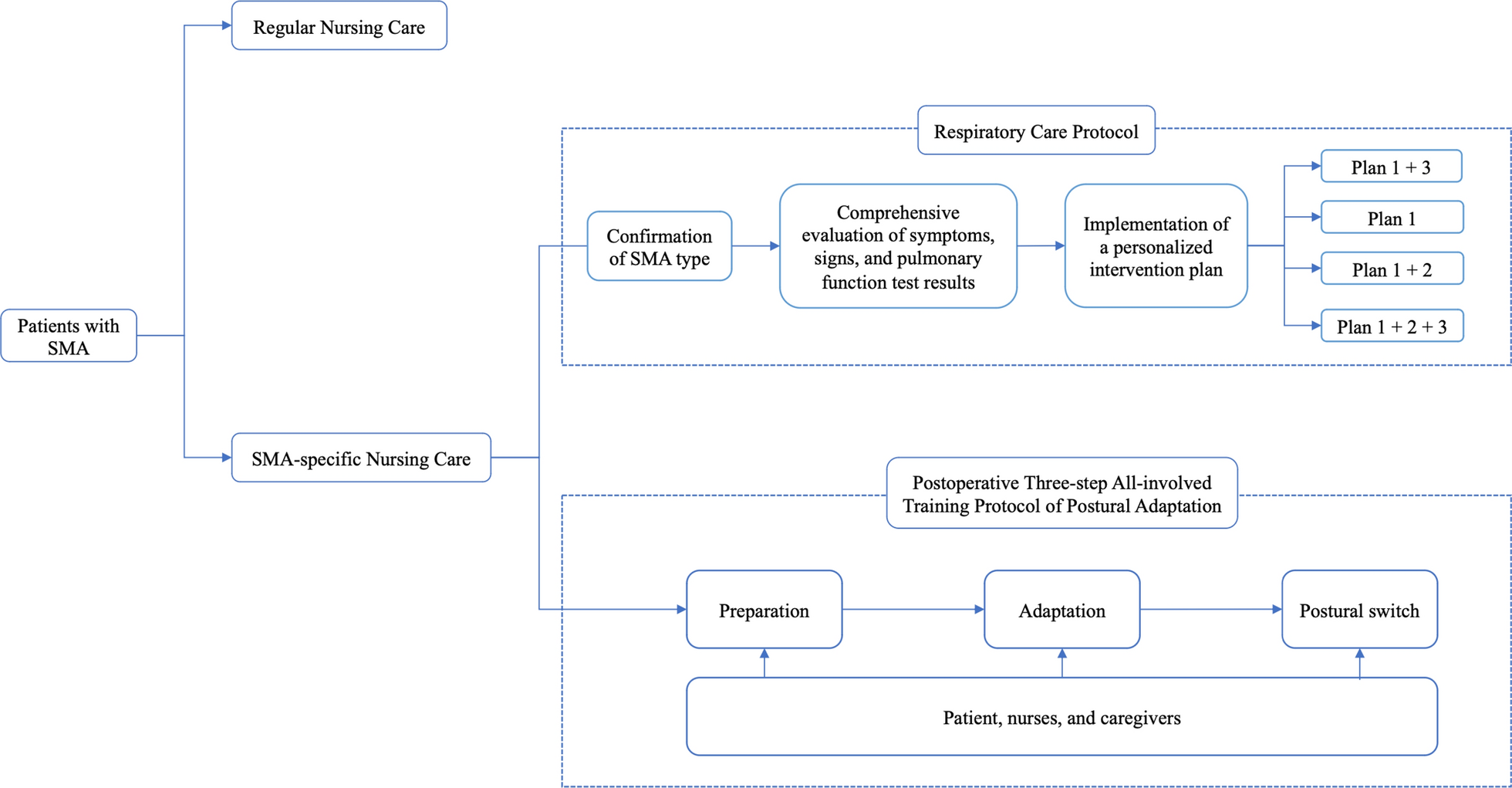
SMA-specific personalized nursing care protocolAn SMA-specific personalized Nursing Care Protocol was developed considering the complexities of SMA. The protocol is summarized below, and an overview of the flowchart is shown in Fig. 1. The SMA-specific personalized Nursing Care Protocol is implemented complementing regular nursing care when a patient with SMA is admitted. The Protocol includes a respiratory care protocol and a postoperative three-step all-involved training protocol of postural adaptation.
Fig. 1
SMA-specific personalized Nursing Care Protocol
1.Respiratory Care Protocol
2.A. Confirmation of SMA type
Pulmonary function is preliminarily evaluated based on the SMA subtype since SMA type III is usually a less severe form.
B.Comprehensive evaluation of symptoms, signs, and pulmonary function test results
In addition to the preoperative pulmonary function test, which is standard practice, special attention is given to a comprehensive evaluation of “symptoms and signs”. It includes the following assessments: recurrent pulmonary infections in the past three months, dyspnea, lung auscultation, sputum accumulation, cough effectiveness, characteristics of sputum, body temperature, and nocturnal hypoventilation. A detailed protocol is available in Supplementary Fig. 1.
C. Implementation of a personalized intervention plan
Based on the results of the above-mentioned evaluation, a personalized intervention is implemented, including one of or a combination of the following three training plans.
Plan 1:Training on respiratory function.
The flowchart of training on respiratory function is shown in Fig. 2. During training, a “sitting position” is adopted to lower the position of the diaphragm and increase lung ventilation. This position helps increase the depth of breathing and the effectiveness of respiratory training. The patient is guided to do a diaphragmatic breathing exercise, which reduces the work of breathing muscles, increases the range of diaphragm movement, and improves ventilation function. The patient is taught to take a deep breath through the nose. Considering respiratory muscle weakness, the patient may be instructed to place his or her hands on the abdomen and inhale during the abdominal bulging to feel the change in strength. The inhalation to exhalation ratio is 1:3–4. Coughing exercise is carried out 10 times each in the morning, noon, and evening. It comprises taking a deep breath, holding it, and then forcefully coughing 2–3 times using the abdominal muscles. Exhalation exercise involves blowing paper through a pursed lip, 10 sets each time, 2–3 times a day. For inhaling exercise, a patient with an FVC equal to or greater than 600 ml is instructed to use incentive spirometers. For a patient with an FVC of less than 600 ml and weak respiratory muscle strength, a “low-resistance breathing trainer” and a passive lower limb treadmill are recommended. When training with devices like POWERbreathe®, the resistance is adjustable. Using an appropriate training load, the patient is instructed to place the mouthpiece in the mouth, and then take a fast, forceful breath in to expand the chest. For exhalation, the patient should breathe out slowly and passively through the mouth to empty the lungs, then pause for about 3–4 s until feeling the urge to inhale again. This training is performed twice a day for 30 times each set, and a training diary is kept to improve patient compliance. If the patient experiences wheezing, dizziness, or coughing during training, he or she is instructed to take a short break. This training process is tolerable for most patients. A passive lower limb treadmill trains the diaphragm to improve respiratory muscle strength and endurance, achieving the goal of inspiratory muscle training. It is performed using lower limb exercise equipment with four movements including “leg pedaling, leg splitting, hip flexion, and leg extension”, 10 times per set, and a total of 3 sets every day. Nurses instruct and evaluate the patient’s tolerance at the bedside throughout the entire training.
Fig. 2
Training on respiratory function
Plan 2:Use of cough assist device.
It is widely acknowledged that patients with type II and type III SMA having difficulty with independent sputum clearance should be evaluated for the use of a cough assist device. Insufflation and exsufflation pressures are adjusted based on the patient’s pulmonary function and sputum clearance ability. The nurse first evaluates the patient’s and caregiver’s understanding and usage of the cough assist device. Then the nurse explains the two phases of the device: during phase one, positive air pressure is applied to expand the lungs and loosen the bronchial secretions; during phase two, negative pressure pushes secretions toward the large airways for clearance by suction. The pressure is typically set at ± 25–40 cmH2O, depending on the subtype and the patient's tolerance. At the same time, the patient and caregiver are instructed to pay attention to: positioning the patient in a semi-recumbent or upright position, stabilizing the neck to avoid cervical instability during suction; clearing oral and nasal secretions prior to using the device, either before meals or at least one hour after meals; performing at least 10 cough cycles in each session, and at least two sessions each day. The patient and caregiver are encouraged to participate together and practice multiple times. A flowchart for utilizing the cough assist device is shown in Supplementary Fig. 2.
Plan 3:Use of non-invasive ventilator.
Non-invasive ventilation treatment is used during nighttime sleep for SMA patients with nocturnal hypoventilation. This includes snoring, waking up due to breathing difficulties during sleep, feeling sleepy and fatigued upon waking up in the morning, and mild carbon dioxide retention as detected by blood gas analysis. A flowchart for utilizing the non-invasive ventilation is shown in Supplementary Fig. 3.
2.Postoperative three-step all-involved training protocol of postural adaptation
The postural adaptation protocol includes three steps and requires participation from the patient, caregiver, and nurses, as shown in Fig. 3 and Supplementary Figs. 4 and 5.
Fig. 3
Postoperative three-step all-involved training protocol of postural adaptation
A.Preparation for the training
The patient should take an active role during the entire process. The nurses explain the detailed protocol to the patient and caregiver, helping them gain a better understanding of the protocol and what to expect from the training. The caregiver is instructed to do a patient-caregiver role switch to appreciate the patient’s experiences and challenges.
B.Postural adaptation training.
In this section, the patient gradually adapts to sitting balance. The training shifts from nurse-led to caregiver-led in a gradual and collaborative manner. The essential elements involve optimizing pelvic alignment, maintaining spinal alignment, progressively increasing head-of-bed elevation and duration while adjusting the plan based on the patient’s tolerance (Supplementary Fig. 4). This approach enhances the patient’s autonomic nervous system modulation and strengthens the paraspinal muscles, facilitating the gradual adjustment to sitting balance.
C.Postural switch from lying to sitting.
This section involves completing the position change with a focus on “safety + comfort” (Supplementary Fig. 5). Before the position change, the patient receives appropriate analgesia. Three nurses work together to complete the postural switch: the nurse near the head of the bed is responsible for the shoulders and waist, the nurse near the foot of the bed is responsible for the lower limbs, and the nurse on the opposite side is responsible for overall assistance and safety. Given the weak head control ability of patients with SMA, the nurse on the opposite side must also support and protect the neck of the patient after sitting to enhance stability and balance. Attention should be paid to any discomfort observed during the position change. Sitting time is gradually increased according to the patient’s tolerance. The training also shifts from nurse-led to caregiver-led. The nurses assess the caregiver’s learning outcomes to enhance their proficiency in long-term home care.
Comments (0)