
Remember me


A 58-year-old male patient presented to the Maxillofacial Surgery Department of the University Hospital of Sassari, Italy, with a left-sided hard palate squamous cell carcinoma extending to the contralateral side (Fig. 1). The participant provided informed consent for the use and publication of their data and image in this manuscript, with a signed consent form.
Fig. 1
Preoperative presentation. (A) Lateral facial profile of the patient. (B) Intraoral view revealing the squamous cell carcinoma lesion involving the hard palate and extending contralaterally
Preoperative clinical examination and imaging studies, including contrast-enhanced CT and MRI, were performed to define the local tumor extent and evaluate for regional or distant metastases. Following the multidisciplinary tumor board review, the patient was scheduled for a total maxillectomy and primary reconstruction with a combined osteomyocutaneous fibula flap and a custom-made, additively manufactured subperiosteal implant.
The planning process for the patient-specific implant and the associated fibula osteotomies was based on the high-resolution CT scans of the craniofacial region (in DICOM format) to assess the maxillary defect and define the extent of bone removal. Optical impressions of the dental arches and a diagnostic wax-up were also obtained to ensure that the final implant would accommodate a suitable prosthetic rehabilitation, mirroring the patient’s ideal occlusion and aesthetic parameters. In addition to the craniofacial scans, CT angiography of the lower limbs was performed. This provided critical information about the vascular anatomy of the fibula and guided the planning of fibular segment harvest and osteotomies.
The acquired DICOM datasets were forwarded to Sintac Biomedical Engineering (GPI group, Trento, Italy). Using Mimics software (Materialise, Leuven, Belgium), the medical imaging data were segmented and converted into an STL file, generating a high-fidelity three-dimensional model of the maxilla and the relevant anatomical structures. During this phase, any artifacts or inconsistencies in the imaging data were addressed to ensure an accurate virtual representation of the patient’s anatomy.
Next, the design of the patient-specific subperiosteal implant proceeded in Geomagic Freeform software (3D Systems Inc., Rock Hill, SC, USA). The implant was virtually adapted to the planned resection margins, factoring in the post-maxillectomy defect that would be created (Fig. 2A). Multiple parameters were considered, including the anticipated positioning and angulation of prosthetic abutments, strategic placement of fixation holes for osteosynthesis screws, and extended arms to accommodate intraoperative variations (Fig. 2B).
Fig. 2
Virtual surgical planning. (A) Three-dimensional reconstruction of the midface and maxilla, highlighting in red the planned resection area for the total maxillectomy. (B) Design of the patient-specific subperiosteal implant (gray) and fibula bone segments (blue). Note the integrated fixation holes and extended arms to accommodate intraoperative variations
Concurrently, the CT angiography of the lower limbs was integrated into the planning. These images guided the optimal harvest site from the fibula and informed the design of patient-specific cutting guides for the bone segments. These guides ensured that the fibula would be segmented precisely as required to fit the newly created maxillary defect. The digital plan defined the length and orientation of the fibular segments and their alignment with the implant framework, enabling a stable and anatomically compatible reconstruction.
Upon completion of the virtual designs, the engineering team presented the comprehensive plan, including the implant, fibula osteotomies, and cutting guide designs, to the surgical team. A collaborative review allowed for iterative refinements, ensuring that the surgical plan was both anatomically accurate and practically feasible. Once approved, the implant was fabricated using direct metal laser sintering (DMLS) technology in a Ti6Al4V titanium alloy. The titanium implant underwent heat treatment to enhance its mechanical properties—improving fracture toughness, thermal stability, and dimensional reliability under load. Selective 3D printing techniques were used to fabricate the fibula cutting guides and anatomical models from high-performance polymers (e.g., polyether ether ketone). The entire cycle from data acquisition to the final sterilized implant and cutting guides took approximately ten days, ensuring no delays in the planned surgery.
Under general anesthesia, the patient underwent a total maxillectomy with intraoperative frozen section analysis to confirm tumor-free margins. The previously planned fibula osteotomies were executed using the patient-specific cutting guides (Fig. 3A), ensuring precise segment preparation. The custom subperiosteal implant was then positioned to provide a stable foundation for the fibula segments (Fig. 3B), which were rigidly fixed with osteosynthesis screws through the integrated design features of the implant (Fig. 3C). Microvascular anastomosis of the fibular pedicle was performed to the facial artery and vein using end-to-end anastomosis. No vascular grafts were required, as the recipient vessels provided adequate pedicle length to ensure a tension-free anastomosis.
Fig. 3
Intraoperative stages of reconstruction. (A) The fibula bone segment with the surgical template used to perform the osteotomies. (B) The custom-made subperiosteal implant fixed onto the fibula flap prior to inset. (C) Intraoral view of the implant and fibular segments rigidly secured with osteosynthesis screws, reconstructing the maxillary defect. (D) Immediate postoperative closure showing proper soft tissue adaptation over the reconstructed area
The fibular flap’s soft tissue paddle was contoured to recreate the palatal surface and re-establish the separation between the oral and nasal cavities (Fig. 3D). Closure was achieved without complication, and the patient was transferred to the recovery ward for postoperative care.
Histopathological analysis confirmed a pT4a squamous cell carcinoma, and the patient subsequently underwent adjuvant radiotherapy. Radiotherapy was initiated six weeks postoperatively to allow for optimal soft tissue healing and to minimize peri-implant mucosal irritation. During the radiotherapy period, the transmucosal abutments remained submerged to minimize mucosal irritation and facilitate healing. After completing radiotherapy, the abutments were exposed, and a provisional prosthesis was delivered, restoring the patient’s masticatory function, phonetics, and aesthetics. Six months postoperatively, once the soft tissues had fully matured, a definitive prosthesis was fabricated and loaded.
At the two-year follow-up, the patient remained alive and free of disease recurrence. Clinical and radiographic evaluations showed stable implant integration (Fig. 4), healthy peri-implant soft tissues, and the absence of any mechanical or biological complications. The prosthetic rehabilitation remained fully functional, contributing to a significant improvement in the patient’s quality of life (Fig. 5).
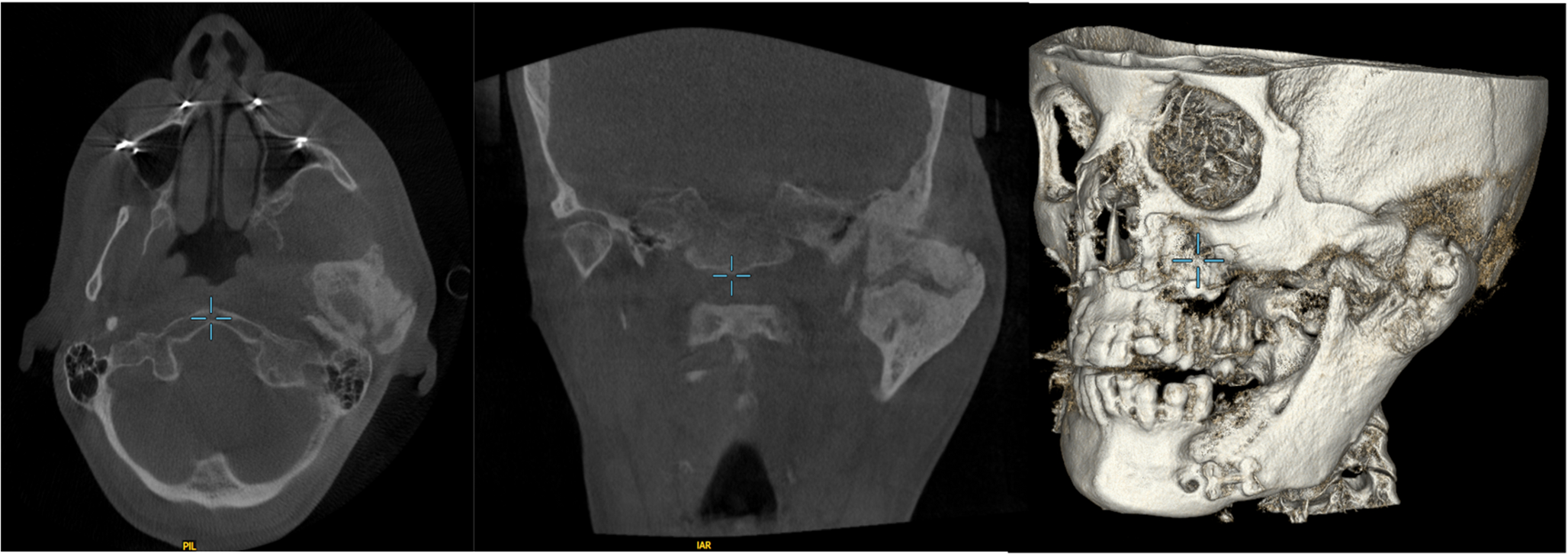
Fig. 4
Post-operative 3D CT scan one year after the surgery
Fig. 5
Two-year postoperative results. (A) Frontal and (B) lateral extraoral views demonstrating symmetrical facial contours, stable soft tissue support, and no external deformities. (C) Intraoral view of the definitive prosthesis fully integrated with the reconstructed maxilla, restoring palatal form and occlusal function. (D) Frontal intraoral view
Comments (0)