Cemento-osseous dysplasia is a well described disease process whereby healthy bone is replaced by sclerotic bone. It is the most prevalent of the fibro-osseous lesions presenting in the jaws. Despite being fairly common in females of African and Asian origin, there is a lack of studies in the literature on COD in African populations [8]. Therefore, this study is one of the largest and most comprehensive on the management of COD in a predominantly African population.
Clinico-pathological features
Middle-aged individuals of African ancestry are the population group most commonly affected by COD. The mean ages of patients diagnosed with COD in the literature ranges from 40.6 to 66.5 years, with an overall mean of 52.2 years [5,6,7, 9,10,11,12,13,14]. Females are significantly more likely to be affected with COD, whereas it is infrequently reported in males. This study’s findings align with these observations. The disproportionate prevalence of COD in females has been hypothesized to be due to hormonal imbalance that influence bone remodelling [15].
Generally, COD is described as an inconspicuous condition, usually detected incidentally on routine radiography. Some affected patients may present with swelling, pain and purulent discharge due to secondary infection in the bone surrounding the lesion. Studies in the literature report the presence of symptoms to range from 14.7 to 100% of cases [5, 7, 9,10,11,12]. In this study, 38.7% of cases were incidentally found on routine radiography.
There is consensus in the literature that the mandible is by far the most affected jaw, with the majority of lesions presenting in the posterior regions of the mandible [6, 7, 9, 10, 13, 14]. In current study’s sample, more than three quarters of CODs occurred in the mandible alone, while 20.2% occurred in both jaws. CODs occurring in the maxilla alone were uncommon.
There is conflicting data in the literature regarding which subtype of COD is the most common. Some studies report focal COD as the most prevalent subtype [6, 10, 14], while others identify florid COD as the most common [5, 7, 9, 11, 13]. In this study, focal and florid CODs were nearly equally common, with focal COD being slightly more prevalent. MacDonald-Jankowski [16] and Pereira et al. [6]. reported that all florid CODs involved the mandible, while nearly half also involving the maxilla as well.
The radiological features of COD are crucial for an accurate diagnosis. The majority of studies in the literature report that COD typically appears as a mixed density lesion on radiographs [6, 7, 9,10,11, 14]. However, studies focusing solely on florid COD have found that many lesions are radiopaque due to their mature nature [5]. In this study, nearly half of florid COD cases (46.4%) appeared radiopaque.
There is general agreement in the literature that CODs appear as well-defined lesions on radiographs in most cases [10]. Alsufyani and Lam [10] reported that 91.5% of CODs in their sample were well-defined. Similarly, in the present study 93.5% of lesions were well-defined. Ill-defined lesions warranted further investigations using advanced imaging or biopsy to rule out more sinister conditions.
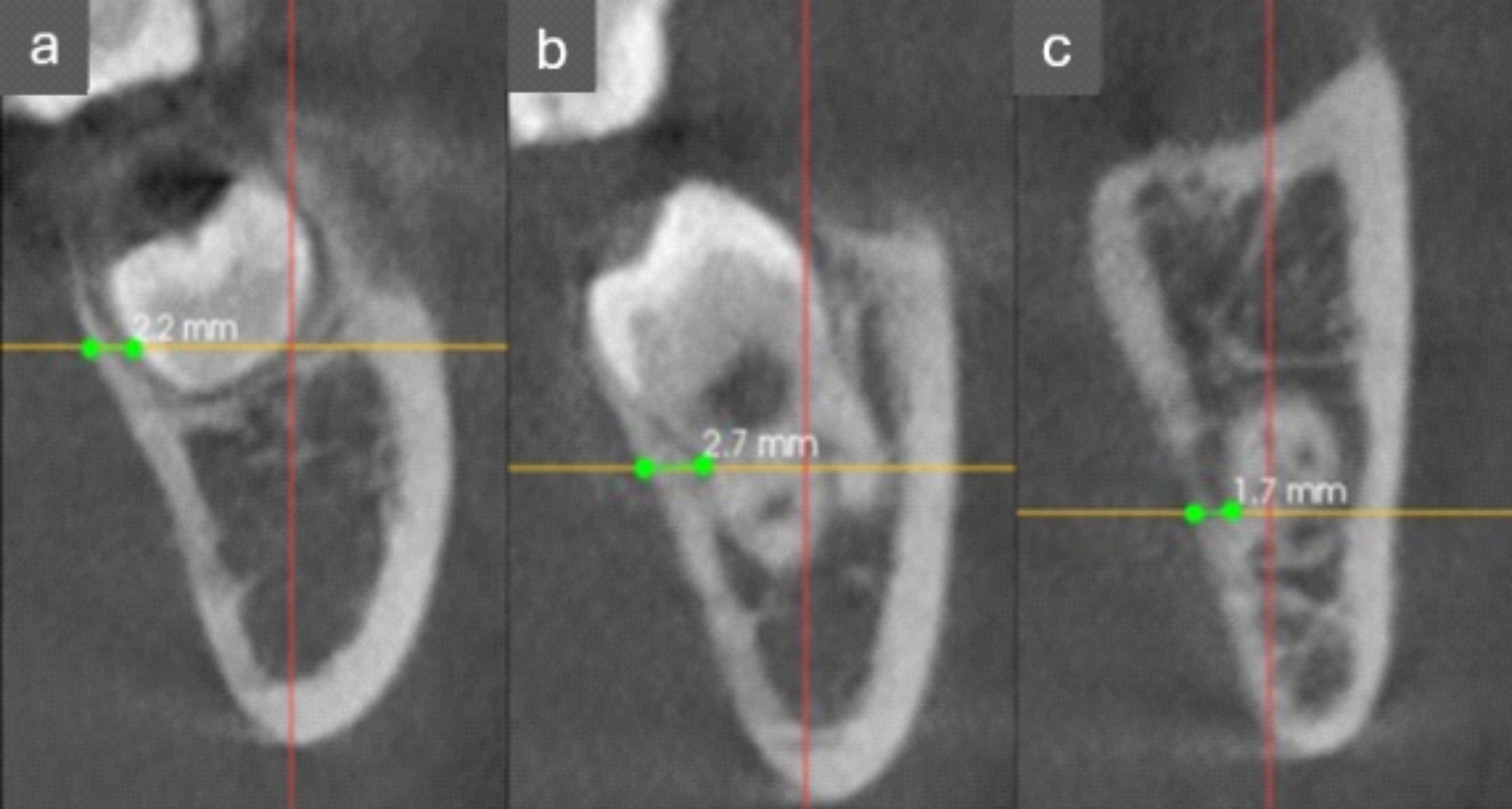
In our study, the relationship of COD with adjacent anatomical structures was assessed using multiplanar CBCT/CT. Cortical bone aberration was the most commonly involved structure in most subtypes of COD, consistent with other studies [17]. Other frequently observed features included cortical bone thinning, expansion, and perforation. As previously reported, florid COD was responsible for most aberrations to the cortical bone compared to other subtypes of COD, further highlighting its aggressive nature [18, 19].
The accuracy of diagnosis of COD based on clinical and radiological examination is vitally important in order to avoid unnecessary biopsy of asymptomatic lesions. Although arriving at an accurate diagnosis may be challenging, it is essential for appropriate management. Ideally, COD should be diagnosed based on clinical and radiographic signs, with biopsies reserved for uncertain cases [6]. In this study, most cases were accurately identified as COD (sensitivity: 83.3%), a finding similar to other authors [10].
Management
There is currently no consensus in the literature regarding when surgical treatment for COD is indicated and which method is most appropriate [7]. Generally, it is accepted that asymptomatic COD does not require surgical intervention beyond close clinical follow-up, preventive measures, and restorative methods to prevent the need for dental extraction and exposure of COD to the oral environment [9, 20].
The findings of this study underscore the necessity of biopsy in some asymptomatic cases to rule out other conditions. A biopsy is indicated if the diagnosis based on radiographic exam is uncertain, especially for lesions in the radiolucent phase or those causing significant bone expansion. Additionally, the presence of a second pathology, such as SBC, should prompt a biopsy to confirm the diagnosis [6]. This also applies to the rare occurrence of associated osteosarcoma, as observed in one of the cases in this study [21].
When COD lesions manifest symptoms, their management becomes more challenging due to development of chronic inflammation and bacterial infection within densely mineralized tissue. It has been described that there is poor penetration of antibiotics due to lack of tissue diffusion deeming them ineffective [6]. Consequently, performing a biopsy increases the risk of developing secondary infection, and removing of such lesions in asymptomatic patients can lead to significant morbidity [20].
Surgical debridement and curettage are recognised as the most appropriate methods for managing symptomatic and infected CODs (Table 3). Despite the challenges associated with treating infected lesions, particularly due to the poor vascularity of the area and increased bone hardness, these surgical techniques have shown effectiveness in treating the majority of infected CODs, with a success rate of 88.9% [7]. Antibiotics play an adjuvant role by inhibiting the formation of new biofilms through the destruction of bacterial colonies before they can adhere to the necrotic bone.
Table 3 Comparison of types of COD and their management in this study with other recent studies in the literatureThe primary prognostic indicator for the development of infected CODs in this study were identified as dental extraction and the use of removable dentures. Kato et al. [7]. reported comparable predictive factors for the onset of infection within COD lesions. Chronic secondarily infected COD were found to be more easily to curettage from the underlying bone, as the osteolytic process leads to the sequestration of the necrotic lesion. In these cases, patients generally exhibit compromised wound healing, precluding the application of bone grafting. Iodoform impregnated gauze has been shown to facilitate wound healing and the formation of granulation tissue. Certain authors have suggested the utilization of local soft tissue flaps, such as buccal fat pad, to aid in wound closure. Should there be a failure to heal after a period of 3 to 4 months, secondary surgical intervention should be considered [12].
Following an extensive literature search, very few studies focused on the management of COD. This study stands out as one of the most comprehensive analysis focused on the treatment of COD. Furthermore, using findings from this study along with data available from the literature, a management protocol is proposed (Table 4).
Table 4 Treatment protocol for Cemento-Osseous dysplasiaComplications
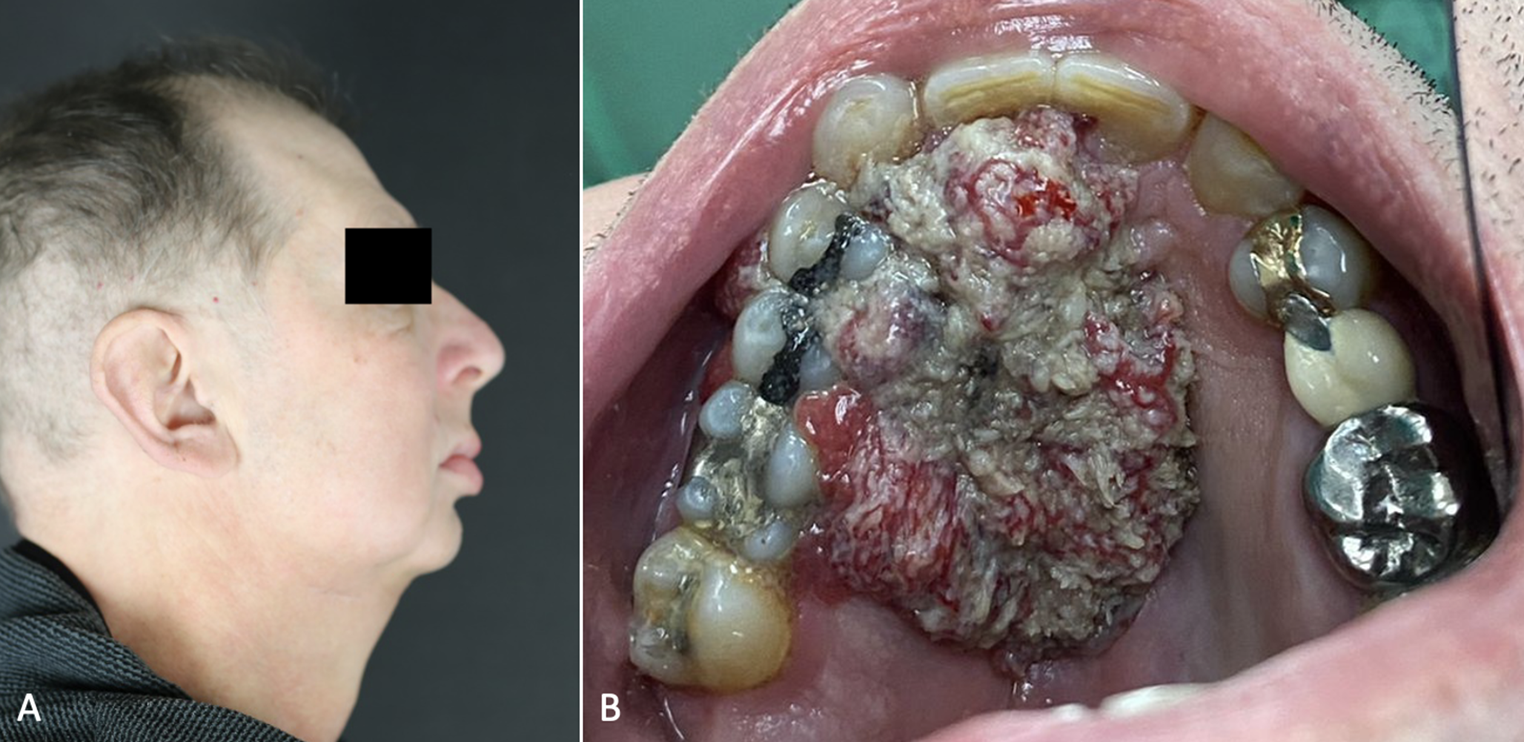
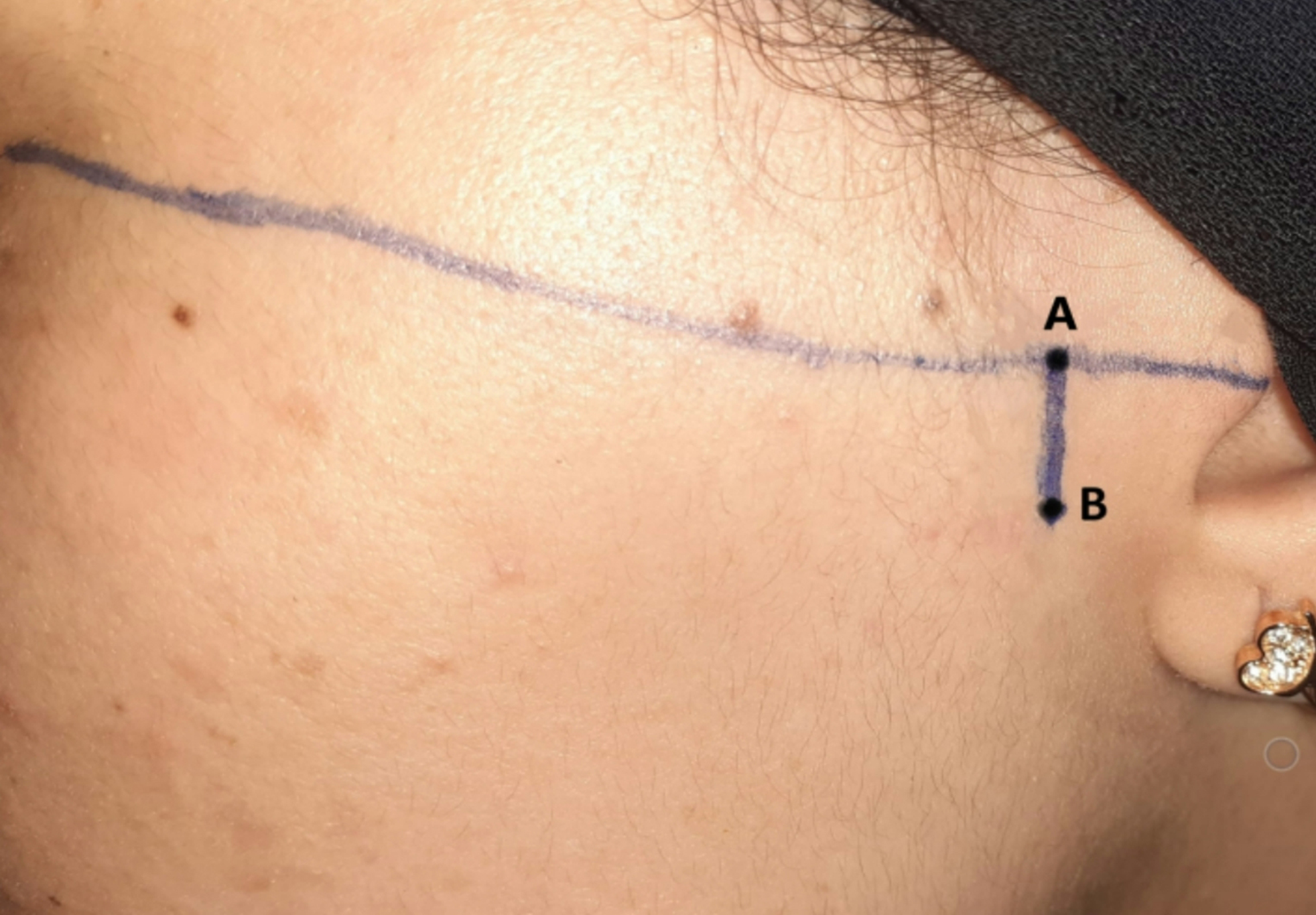
One of the major complications associated with COD is the development of osteomyelitis, especially in the mandible, which leads to high morbidity for the patient and development of cutaneous fistulas, as seen in this sample. Elbeshir and Alhadad [9] reported that 25.5% of their Sudanese sample to have developed osteomyelitis, while Alsufyani and Lam ([0] reported an 11% prevalence. Kawai et al. [15]., in a Japanese study, reported a 14.8% prevalence, whereas in this study, only 5.6% of patients developed osteomyelitis. This lower rate of osteomyelitis in this study is likely due to aggressive and early surgical intervention in infected CODs cases to prevent progression to osteomyelitis. Elbeshir and Alhadad [9] managed most COD cases in their sample with antibiotics initially, while only refractory cases were treated with surgical debridement. This approach may explain the higher prevalence of osteomyelitis in their study when compared to this one.
The recurrence rate and need for surgical re-treatment of COD is another possible complication. Nam et al. [14]. reported excellent outcomes following surgical removal or curettage and administration of antibiotics, with no recurrence. In the current study, three cases (2.4%) required re-treatment due to incomplete removal. The decision for incomplete removal was initially made to avoid injury to vital structures, such as the inferior alveolar nerve.
Several limitations were encountered in this study, which are commonly encountered in other retrospective record-based studies. A significant number of records (approximately 12%) did not meet the study’s inclusion criteria due to missing information. For some older records, it was challenging to attain the patient’s clinical presentation due to incomplete record keeping. Given that the study was conducted over a period of 18 years and at two different hospitals, treatment methods could not be standardized, as multiple providers performed these procedures during this time period. Additionally, a significant number of patients were lost to follow-up, as many lived in rural communities far from these hospitals.
In conclusion, the decision to surgically manage COD lesions should be based on clinical signs and symptoms, as well as the presence of infection or osteomyelitis. Asymptomatic cases should be monitored periodically, with an emphasis on preventative measures to avoid secondary infections. Biopsy of asymptomatic lesions should only be performed when the clinico-pathological features are inconclusive and lesion could mimic other more sinister conditions. The presence of pain, suppuration and osteolytic changes with or without bone sequestration, are indications for surgical intervention in infected COD. Despite the lack of consensus regarding treatment regime, early curettage or surgical excision of infected COD is the most successful approach to eradicate the disease process and prevent further progression into osteomyelitis.





Comments (0)