The bursa is a small pouch between articular region tissues, such as the tendon, bone, and skin, which reduces friction between them [1]. Bursitis occurs when the bursa becomes inflamed [1,2,3]. Common onset sites are joints, such as the elbow and knee, and other articulation-relation regions, such as the trochanteric region and posterior calcaneus [2, 4–5]. Trauma is the most common cause, but other causes include infection, inflammatory arthritis, such as gout or rheumatoid arthritis, and chronic mechanical irritation [8]. In chronic bursitis, swelling is often present but pain is absent [1]. Bursitis is typically examined by radiography, ultrasonography, MRI, or microbiology via aspiration. It is difficult to differentiate between infectious and noninfectious bursitis on the basis of clinical and imaging findings, and microbiology via aspirationcons is required if the possibility of infection remains [2]. The treatment of bursitis can be divided into conservative and surgical treatment. Conservative treatment includes rest, needle aspiration, and steroid injections [1,2,3,4]. Steroid injections may reduce inflammation and symptoms, but the recurrence rate is high [4]. Sclerotherapy is also effective for treating bursitis [3, 5]. Surgical treatment is considered in cases of recurrent bursitis or if conservative treatment has an incomplete effect [1–2, 8].
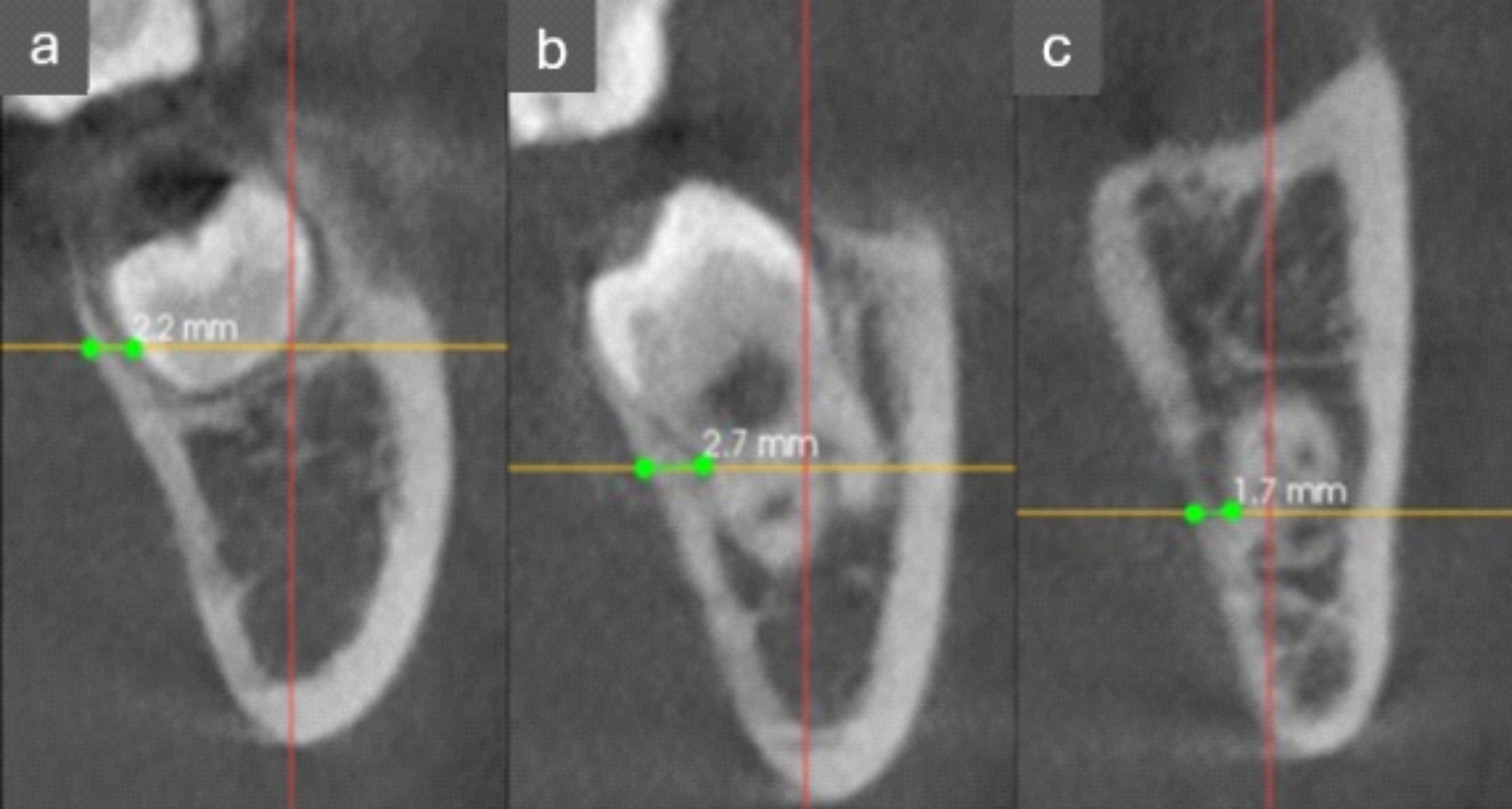
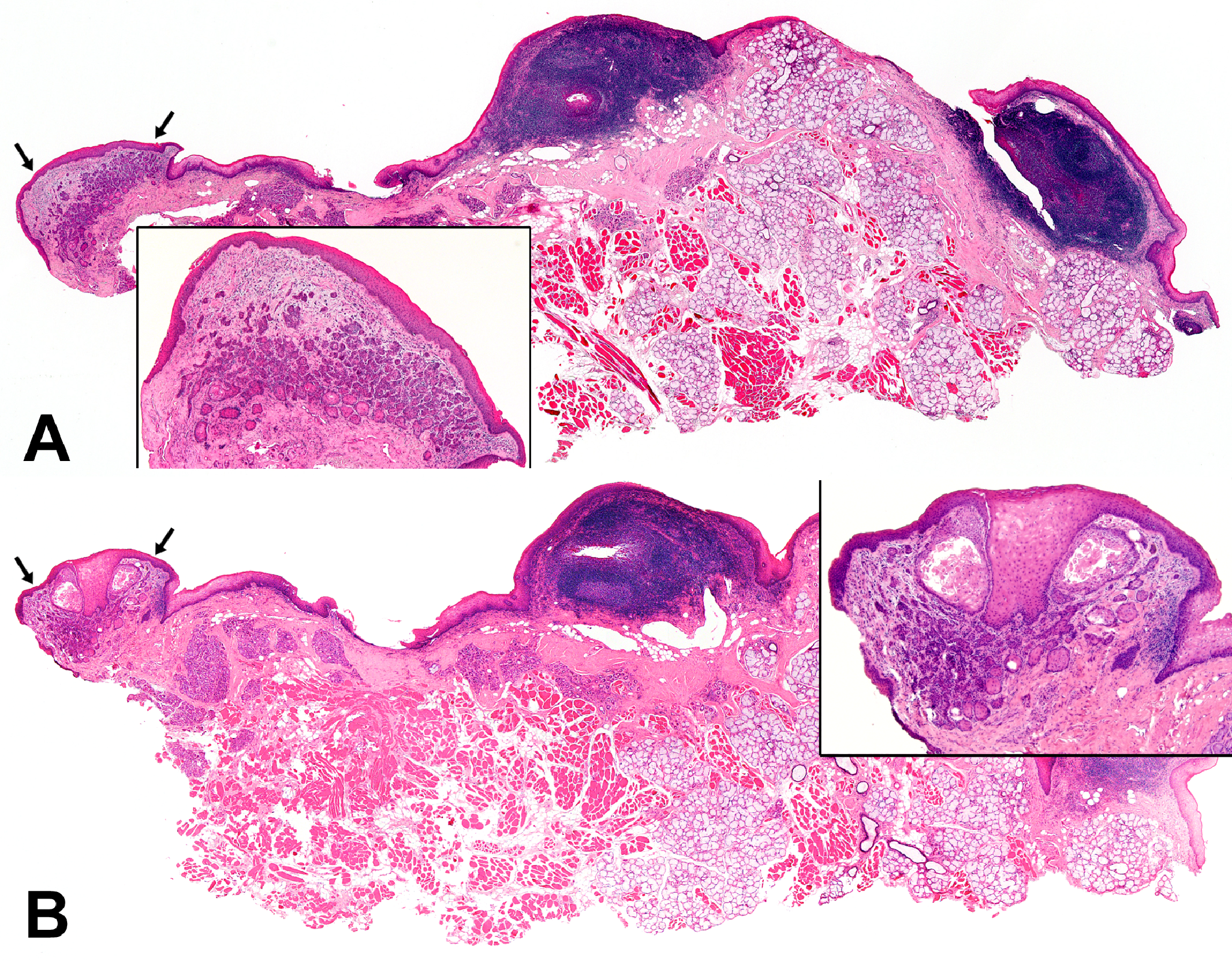
Differential diseases in this case included lipoma, dermoid cyst, ganglion, soft tissue tumors such as synovial sarcoma and fibrosarcoma, salivary gland tumors such as pleomorphic stroma and adenoid cystic carcinoma, osteomyelitis, and lymphoma. In the present case, MRI showed a cystic lesion with a thick membrane, needle aspiration showed no evidence of malignancy with a liquid interior, and histopathology showed synovial cell lining and immunohistochemistry was positive for vimentin and the presence of synovial cells, leading to the diagnosis of bursitis.
In this case, bursitis occurred in the nonarticular part of the mandible, and there have been no previous reports of bursitis occurring in the same region. Lee et al. reported bursitis in the temporomandibular joint after reduction malarplasty and concluded that it was caused by inflammation or intraoperative damage to the joint capsule [9]. Thukral et al. also reported pterygoid hamulus bursitis that was caused by extensive medial deviation of the pterygoid hamulus [6–7]. Salvarani et al. noted an association between active polymyalgia rheumatica and cervical interspinous bursitis [10]. The region where bursitis arose in the present case did not include a bursa. There were no findings of inflammatory arthritis or infection; therefore, it was unlikely to be a region of chronic mechanical irritation, and trauma was the most likely cause of the bursitis. AD was suspected as the cause of the trauma.
AD is a common inflammatory skin disease associated with itching. It is a combination of various factors including genetic predisposition, environment, and epidermal barrier dysfunction. Cytokines are produced by activated lymphocytes and other inflammatory cells due to epidermal barrier dysfunction, resulting in persistent inflammation [11]. Nassif et al. reported the occurrence of bursitis of the olecranon and anterior tibia during dermatitis flares in patients with AD, suggesting an association between the two conditions [8]. Severe AD consistently presents with itching and chronic trauma, such as rubbing and scratching. This trauma can cause bursitis [8]. Leung reported a case of worsening prepatellar bursitis during three asthma attacks [12]. He suggested that the hypoxia caused by asthma may result in the release of enzymes from damaged lung tissue, leading to bursitis. Kim et al. reported a case of subscapular bursitis as an initial manifestation of dermatomyositis [13]. They suggested that this patient’s bursitis may be mediated by autoimmunity, similar to the bursitis observed in rheumatoid arthritis. Although AD and asthma are allergic diseases and not autoimmune diseases, allergy itself is an abnormality of immune function and induces chronic inflammation. Inflammatory cytokines are involved in AD, asthma, and bursitis, and a common pathophysiology may be established. Therefore, we consider another mechanism by which inflammation in AD may be transferred to synovial cells, causing thickening of the synovial membrane and increased internal fluid production, which may form the basis for the inflammatory response observed in bursitis. Regardless of the mechanism, continuous appropriate treatment and disease control will reduce the risk of chronic trauma, such as scratching, and persistent inflammation that can lead to the development of bursitis. In this case, treatment for AD prevented a second recurrence of bursitis, suggesting an association between them.
The present case of refractory bursitis was surgically treated. Although sclerotherapy can be used, the sclerosing agent may damage the facial nerve. In our case, bursitis and AD were treated simultaneously with the goal of curing the bursitis completely by surgery.





Comments (0)