
Remember me




The current study was conducted at the Periodontology clinic, Department of Oral Medicine and Periodontology, Faculty of Dentistry, Mansoura University. The participants were selected from the patients with missing teeth and attending clinic to receive dental implants. The study design was approved by the Ethical Committee at the Faculty of Dentistry, Mansoura University (Reference number: A11100221), and this clinical trial was registered at ClinicalTrials.gov (Identifier: NCT06238427). Written informed consent was obtained from all participants before their involvement in the study. This study was conducted following the Helsinki Declaration for the ethical principles for research involving human subjects.
Patients’ selectionWe carefully selected the participants of the current study according to the following criteria. We included patients requiring dental implants with KMW less than 2 mm at the proposed implant site, and patients who were aged 21 years or older with no systemic condition that affects the implant or grafting surgery. In addition, the following criteria were required; a buccolingual bone width of at least 5.5 mm, a mesiodistal distance of at least 7 mm between adjacent teeth in a single edentulous space, a minimal bone height not less than 10 mm, a well-formed residual alveolar ridge covered with firm mucosa, absence of signs of periodontal bone loss or significant soft tissue loss in teeth adjacent to the implant site, and adequate inter-arch space exceeding 7 mm.
The exclusion criteria were employed to exclude uncooperative patients, Patients with abnormal parafunctional habits, e.g., bruxism and clenching, and Patients who have a systemic or local illness that would disrupt healing. Patients receiving systemic corticosteroids or any other drug that may affect osseointegration or post-operative healing. In addition, smokers with more than 10 cigarettes/day were excluded.
Random distribution of the participantsThe participants were randomly allocated into two groups using computer generated list of randomizations with a randomization table using SPSS V23.0. Both groups received submerged dental implant protocol and FGG. Group 1 received FGG 2 months before placing the dental implant while group 2 received the FGG at the phase of second stage implant surgery.
In addition, each patient received a number from the randomization list, and it was placed in a sealed opaque envelope while the participants were blinded by the treatment protocol and the envelope was opened immediately before surgery. A single-blinded outcome assessor performed all the periodontal and radiographic assessments. This assessor was blinded by the treatment protocol and the allocation of patients into the two groups.
Preoperative patient assessmentComplete medical and dental histories were recorded for all patients and complete clinical intraoral and extraoral examinations were performed. Selected patients were questioned about the cause and time of extractions, whether extractions were because of periodontal disease, dental decay, or other causes. Previous experiences with dental procedures were also discussed. Intraoral photographs were taken to record the existing condition of teeth and mucosa before implant placement. The density and bone levels at the implant site were assessed by CBCT. Consequently, the proper implant size was selected and placed in the ideal position.
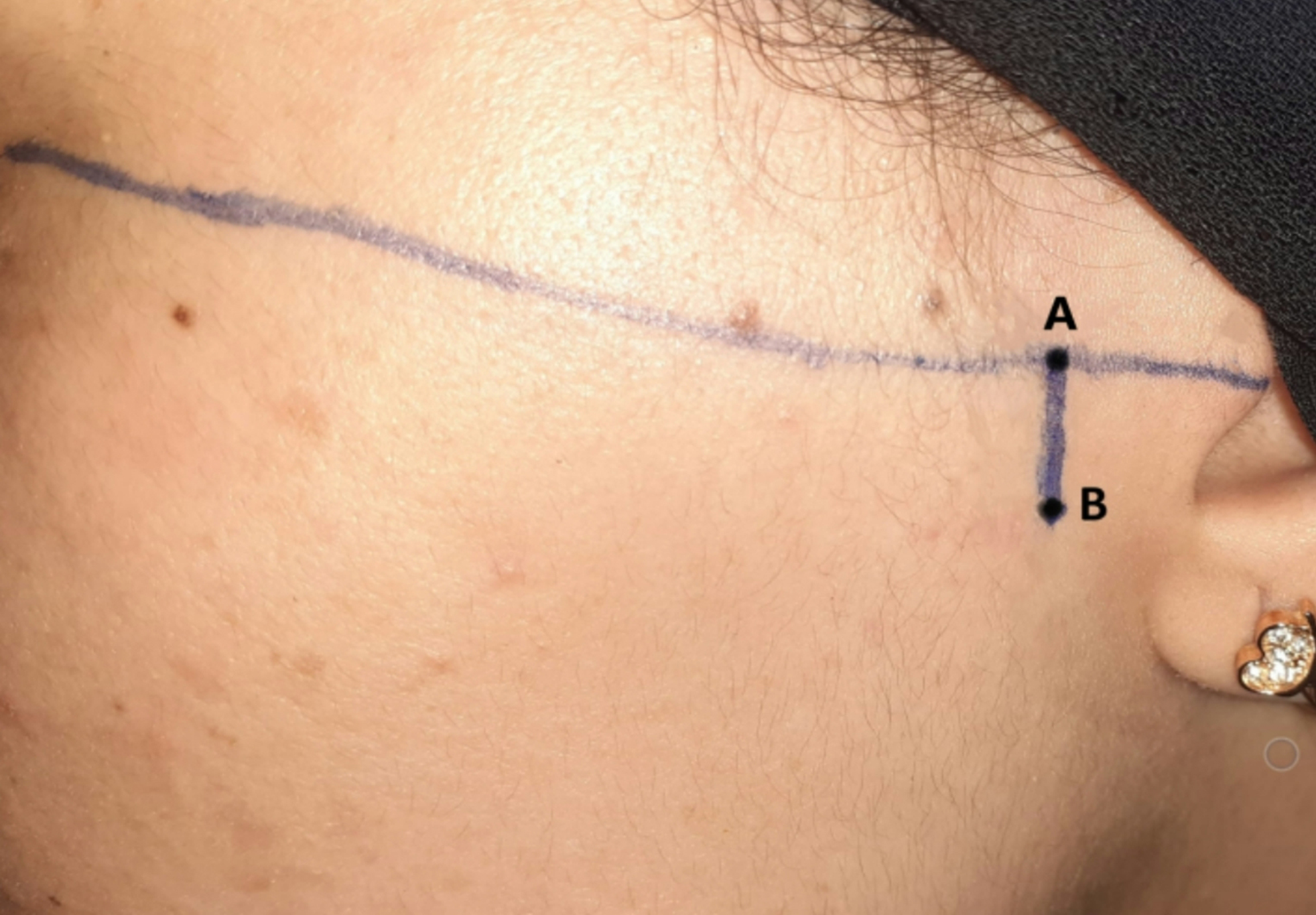
At baseline, periodontal and gingival conditions were evaluated for each patient including the following parameters: KMW and STT. The KMW was measured from the zenith of the alveolar ridge to the muco-gingival junction (MGJ) using a calibrated periodontal probe. MGJ was located using a functional test which is a reproducible method for keratinized gingival width assessment by stretching the lip and cheek or by placing a probe horizontally in the vestibule and rolling to the mucosa coronally, the MGJ is where the mucosa stops rolling or moving.
STT was determined 1.5 mm apical to the soft tissue margin (STM) with a short anesthesia needle or endodontic micro-opener with a silicon stopper. The needle was inserted perpendicular to the mucosal surface, through the soft tissues with light pressure until a hard surface. The silicon stopper was then placed in tight contact with the soft tissue surface with its coronal border overlapping the STM. Then the penetrated part was measured on the endodontic ruler and measurements were rounded to the nearest half of a millimeter.
Intervention proceduresFirst stage surgeryAll the surgical procedures were performed by the same periodontist to standardize the procedures. Before starting the surgery, patients were asked to rinse their mouths with chlorhexidine gluconate for 1 to 2 min to decrease the bacterial load around the surgical site.
After administration of local anesthesia, a mesiodistal mid-crestal incision was made at the proposed implant site where a full mucoperiosteal flap was elevated to the MGJ buccally and lingually. After that, a large round bur was used to recontour the narrow ridge and remove the granulation tissue from the bone in the implant site. Drilling was started carefully to calculate the depth for each implant using the pilot drill. A periapical x-ray was done with the pilot drill in place to evaluate the direction and depth of the drilling in relation to the roots of the neighboring teeth and to vital structures. A parallel pin was placed in the prepared hole to check the alignment and parallelism of future implant position in relation to the neighboring teeth. Sequential drilling was then continued to prepare the site according to the selected implant size. Copious irrigation with cold saline was done during the surgical procedure to avoid overheating of bone which causes bone necrosis and increases the risk of failure. The used implant was an acid etched, tapered, with internal helix connection titanium dental implant (Neobiotech IS II active dental implant).
A torque wrench and an insertion tool were used to insert the implant. A torque of at least 35 to 40 N-cm was obtained, ensuring the implant’s initial stability. The implant was installed at the site of the osteotomy, submerged under the margin of the crest by 1 mm. The cover screw was screwed to the implant, the surgical site was thoroughly irrigated with sterile saline to remove debris and clean the wound and the flap was approximated and sutured using 5\0 monofilament suture.
Second stage surgeryThe second stage of surgery was conducted 2 to 4 months after placement of the implant. Local anesthesia was administered, followed by an incision for the exposure of the cover screw. Any hard tissue overgrowth was removed using a small rose head bur, and the cover screw was taken out. Then, the solid non-customized healing abutment of suitable size and length was connected to allow its emergence through the soft tissues, which was confirmed by a periapical X-ray. Suturing around the healing abutment was performed using a 4/0 non-resorbable suture. The patients were prescribed mouthwash, analgesics, and oral hygiene measures.
Recipient site preparation for FGGIn group 1, the recipient site was prepared 2 months prior to placing the implant. A horizontal incision was performed at the MGJ level along the recipient area’s length. Vertical releasing incisions, slightly divergent toward the sulcus depth, were performed at both mesial and distal ends. Utilizing scalpel 15c, a partial-thickness flap was raised, preserving the nonmobile, firm periosteum connected to the underlying bone to maintain blood supply to the graft. The repositioned flap created space for the graft, free from muscle tension. Careful suturing with 6/0 non-resorbable suture (Proline, Ethicon, USA) stabilized the borders and base, and tin foil paper was trimmed to the graft’s size and validated at the recipient site.
In group 2, the horizontal incision was done at the second surgical stage. It was incised along the length of the recipient area at the MGJ. Subsequent steps in grafting were performed similarly to Group 1. Using a sharp blade, tissues were dissected sharply lingual to the incision line ensuring thorough cleaning of the implant head. Any hard tissue overgrowth was removed using a small round bur. Following the connection of the healing abutment, a periapical X-ray film was taken to verify its complete seating (Figs. 1 and 2).
Fig. 1
Photographs of case from group 1 receiving FGG 2 months prior to implant placement. This graph shows: (1) Horizontal incision along MGJ (2) Partial thickness flap elevation (3) Tin foil adjustment on the recipient site (4) The graft was sutured in recipient site. (5) Acrylic stent in place. (6) Initial healing of the graft (7) Implant installation in the osteotomy site. (8) Healing abutment installation in the 2nd stage surgery, 3 months after implant placement. (9) Periapical x ray with healing abutment in place. (10) Final prosthesis
Fig. 2
Graphs for a case from group 2 with FGG done at time of second stage surgery of dental implant. These graphs show: (1) Preoperative view of the proposed implant site (2) Implant installation with hand wrench (3). Periapical x ray after implant installation. (4) The implant in the osteotomy site. (5) Sutured flap site. (6) Horizontal incision along MGJ. (7) Tin foil adjustment on the recipient site. (8) The FGG harvested from the palate. (9) The graft was adapted in the recipient site. (10) The graft was sutured. (11) Emergence profile. (12) Assessment of KTW gain
FGG harvestingThe FGG was harvested from the hard palate using a tinfoil template in the area bounded by the canine and the maxillary first molar. The depth of the incision was 2 mm. The graft’s edge was gently elevated by tissue forceps and the scalpel was used to carefully detach the graft from the palate (Fig. 3).
The graft was subsequently immersed in isotonic saline and placed on a wet sterile gauze. A surgical gel foam sponge was applied to enhance hemostasis. Then the surgical site was covered with a prefabricated acrylic palatal stent. Suturing was achieved with 6/0 non-resorbable proline sutures. Following the suturing process, finger pressure was applied using wet sterile gauze over the graft for five minutes. This was done to ensure intimate contact and eliminate any potential dead space between the graft and the vascular bed of the recipient site (Figs. 1 and 2).
Fig. 3
Harvesting the FGG from the palate
Prosthetic phaseIndirect impression for the implants was performed by closed tray impression technique as follows: Healing abutments were unscrewed from the implants and impression transfers were installed instead. The impression was taken with elastomeric impression material and closed tray impression technique. After material setting, the impression was removed from the oral cavity, impression-transfer unscrewed from the implant and the healing abutment applied back in place.
Impression transfers were connected to the implant analog to form one unit assembly then the assembled components were seated carefully to their representative place in the impression.
The impression was sent to the lab with a suitable prosthetic abutment for crown fabrication. Then the crown was checked and cemented using glass ionomer cement.
Clinical assessmentKMW, STT, and graft shrinkage were assessed at the following times: baseline, after initial healing of the FGG (7 days after FGG), one month after FGG, 3 months after FGG i.e. one month after implant placement (for group1), one month after implant loading (for group2), 6 months after FGG i.e. one month after implant loading for (group1) and four months after implant loading for (group2) and nine months after FGG i.e. four months after implant loading for (group1) and seven months after implant loading for (group2).
The shrinkage percentage of the gingival graft was measured at 1, 3, 6, and 9 months after the initial healing of the graft. First, the surface area of the graft was determined by multiplying the length by the width. All the measurements at follow-up points of time were compared to the measurement after the initial healing to calculate the shrinkage percentage [19].
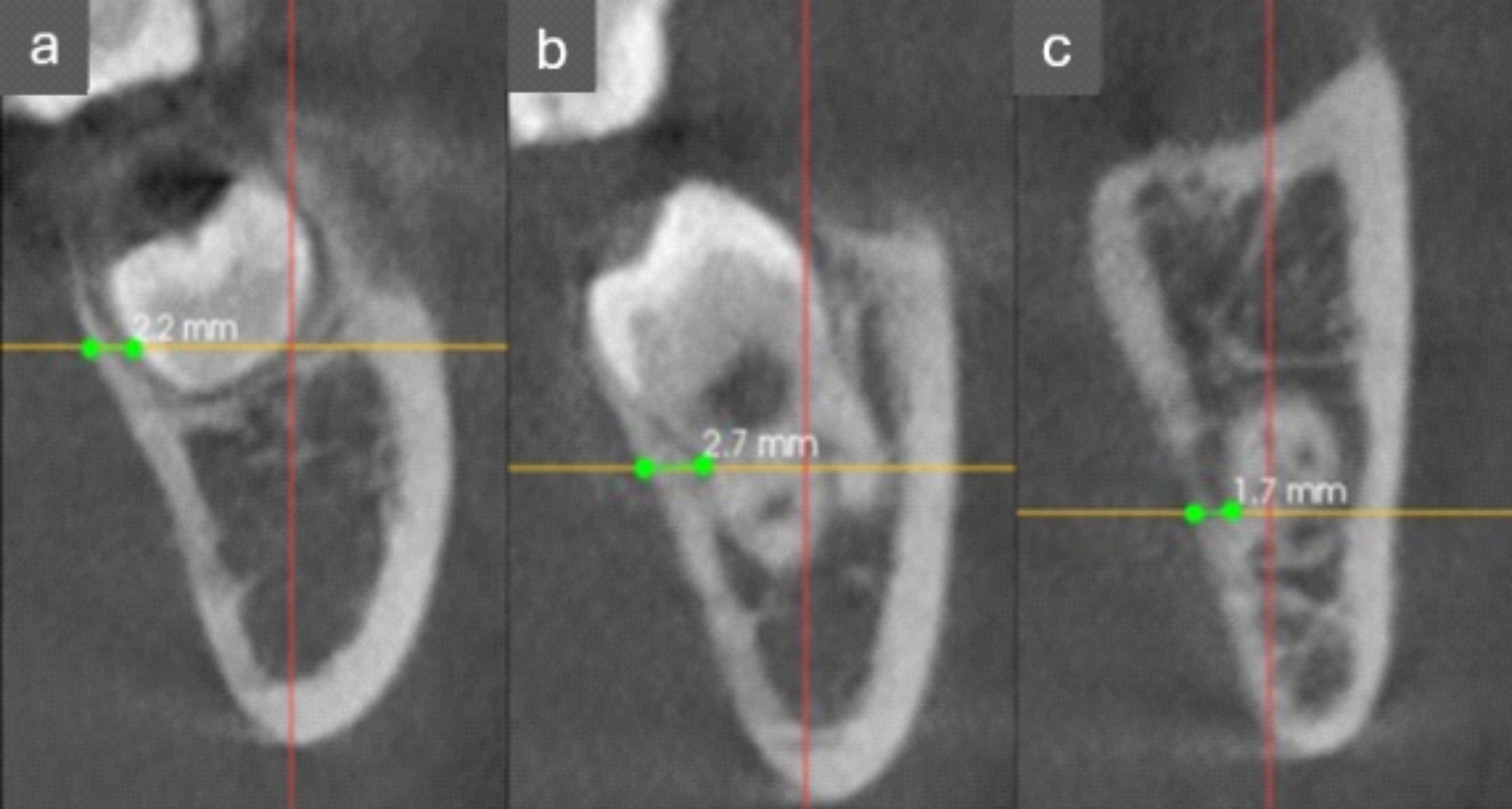
Radiographic assessmentAfter the implant placement in group 1 and 3 months after the second stage surgery in group 2, the radiographic assessment was performed using periapical X-ray with paralleling technique to evaluate the bone level around the dental implant. Analysis of the X-ray was done by the Clear Dent program to measure the distance between the implant collar and the bone level.
Sample size calculation and statistical analysisThe sample size was established using the null hypothesis, which stated that the results of the first and the second groups were not equal. The desired study power was 95% with a confidence interval of 95%. 18 patients were deemed to be the necessary sample size using the G power software (version 3.1.9). The study’s sample size was raised to 20 patients (10 in each group) to account for potential candidate attrition without the potential for altered results. Data calibration was performed before the start of the study to ensure the reliability of the measurements. Sample analysis involved evaluation of clinical and radiographic outcomes at different follow-up times.
Data entry and statistical analyses were done using SPSS version 16.0 (Inc., Chicago, IL, USA). Data were first tested by Shapiro-Wilk test for distribution of data. The mean and standard deviation were used to express parametric data. An Independent t-test was done to compare two means in the study groups. The statistical analysis was performed based on significance level of 0.05 alpha error to reject the null hypothesis.
Comments (0)