This case series aims to analyze computed tomography scan features, examine the timeline of SSS development, and identify factors contributing to its onset. Our findings reveal that most secondary SSS cases develop in the first three months after trauma or surgery. A notable radiological feature in patients who develop SSS after trauma or orbital surgery is the presence of combined orbital fractures involving the orbital floor and medial wall, including the inferomedial strut.
This cohort reflects a predominance of male patients (66,7%), likely due to their greater exposure to physical injuries, as noted in previous trauma research [7]. The time between trauma or surgery and the onset of SSS symptoms ranged from one to thirty-six months, consistent with existing literature [2, 6]. As a tertiary referral center, we expect there will be some delay in referral, suggesting that clinical signs of SSS may have been present for some time before patients had access to specialized care. Additionally, it remains debatable whether SSS occurring many years later can still be attributed to the initial trauma. The median time to presentation in posttraumatic patients is three months. These findings emphasize the importance of follow-up after trauma, even for simple fractures not requiring surgery, particularly those close to the maxillary ostium. Imaging is essential when unexpected changes in globe position and/or an increased Hertel difference are observed. Early detection and intervention are critical to prevent progressive functional and cosmetic deficits.
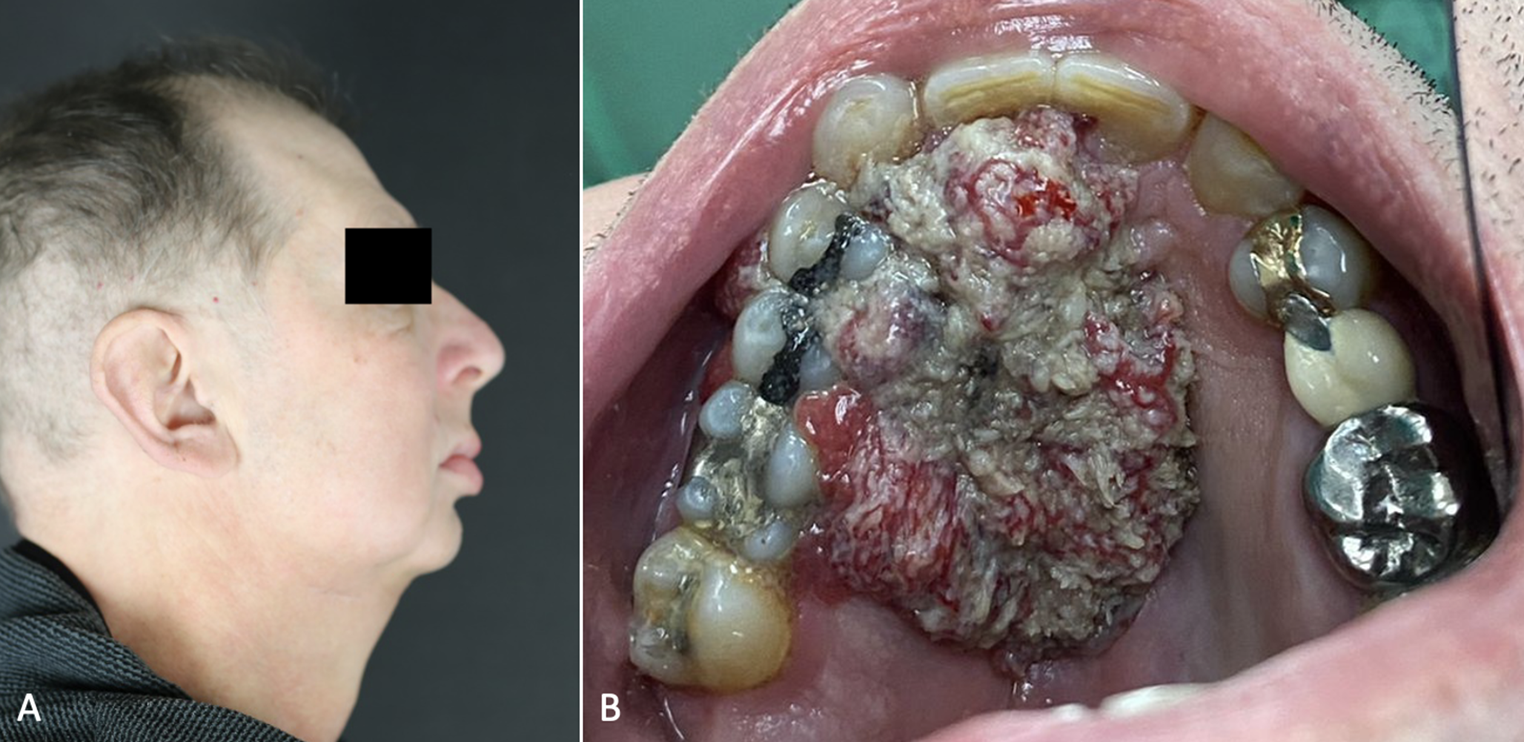
In contrast with other studies [5, 8], diplopia was a presenting symptom in all but one patient, consistently appearing in conjunction with enophthalmos and hypoglobus. Patients with diplopia exhibited more pronounced hypoglobus and enophthalmos than those without it. Hypotropia, limited upgaze, and vertical diplopia were seen in most patients. Given that diplopia tends to develop as orbital dystopia progresses, this pattern likely reflects a delayed diagnosis of secondary SSS in our cohort. This delay may be attributed to the tertiary referral nature of our department, as some patients had already consulted other specialists before being referred to us.
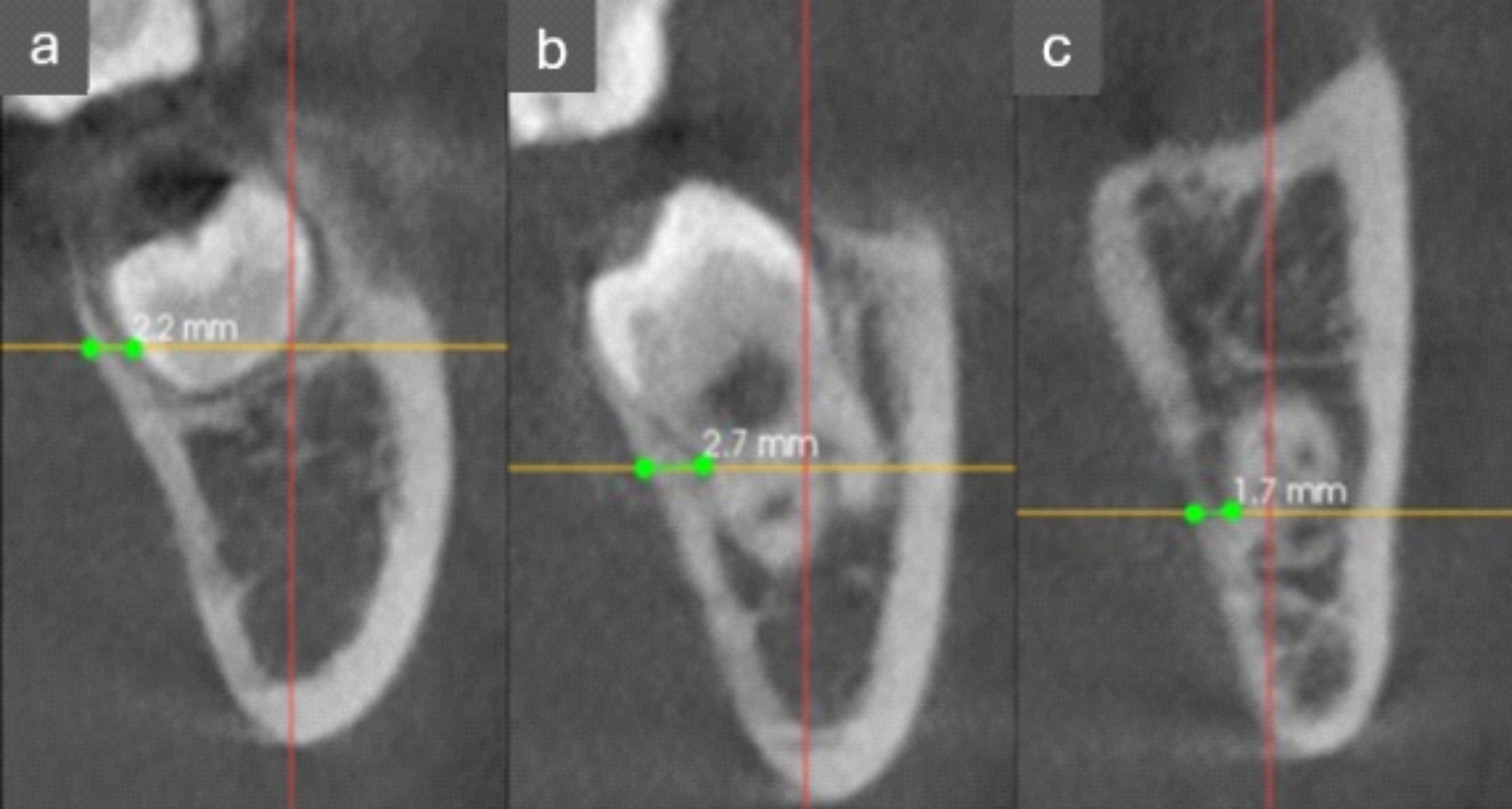
Previous studies on secondary SSS lack information on the posttraumatic/postsurgical imaging showing no signs of SSS. The absence of immediate post-traumatic imaging in published cases makes it challenging to pinpoint the exact moment the syndrome begins to develop, raising questions about the underlying mechanisms and predisposing factors. In our group, the diagnosis of secondary SSS was confirmed by post-traumatic or post-surgical CT scans showing no signs of sinus pathology. Further imaging analysis revealed that fractures involving the orbital floor, inferomedial strut, and maxillary sinus ostium were consistently identified in pre-SSS imaging. These findings align with the theory that obstruction of the maxillary ostium leads to progressive negative pressure, sinus collapse, and orbital floor displacement, contributing to the development of SSS [8, 9].
Although involvement of the maxillary ostium is commonly associated with orbital floor fractures or combined fractures of the floor and medial wall, the development of posttraumatic SSS is still rarely reported [2, 10]. This suggests that a disruption of normal sinus function and anatomy is likely a critical factor in the development of this pathology. However, the underlying factors that trigger the development of SSS in cases of orbital trauma remain unclear. The authors hypothesize that the current trend toward a more conservative approach in orbital fracture treatment [11, 12], may inadvertently increase the risk of secondary SSS. Despite this, the rarity of this condition does not warrant surgical intervention in the absence of clinical indications for orbital fracture repair. Acknowledging the risk of secondary SSS and advising patients to seek evaluation if they experience symptoms or concerns is essential for timely management.
In our cohort, all patients underwent surgical treatment for their SSS, with (retrograde) uncinectomy and orbital reconstruction being the most frequently performed procedures. The decision to proceed with orbital reconstruction was based on the patient’s functional and aesthetic complaints. A single-staged approach was mostly used in cases of significant enophthalmos and diplopia. In contrast, the two posttraumatic cases treated solely by restoring natural sinus ventilation showed no improvement in diplopia or eye position. As a result, a second surgery with orbital reconstruction was performed, leading to the resolution of the symptoms. This suggests that although restoring sinus ventilation is important, it may not be sufficient in cases with clear orbital symptoms.
For cases with mild enophthalmos without diplopia, a two-step surgical approach may be considered, as some patients do not require orbital floor reconstruction or may opt out of further surgery if the altered eye position is not functionally or cosmetically disturbing [5, 8]. Although there are no strict criteria for selecting between a one- or two-stage procedure, our experience suggests that a single-stage approach is often effective. SSS is not a primarily infectious process, and in our series, no postoperative infections occurred with PEEK implants. Therefore, delaying orbital reconstruction solely out of concern for infection may not be necessary. Ultimately, all patients achieved satisfactory outcomes, with restored orbital anatomy and resolution of symptoms.
This study is limited by its small cohort size, which prevented statistical analysis and limited the generalizability of the findings. Further research is needed to identify specific factors contributing to secondary SSS development. Prospective studies incorporating routine post-trauma or post-surgical follow-up would provide valuable data on the early detection and progression of the syndrome. Additionally, exploring the role of individual patient factors, such as anatomical variations, sinus mucosal health, or genetic predispositions, could enhance our understanding of why some patients develop SSS while others do not.





Comments (0)