Study setting
The study was conducted in Guangua (population 110,066) [19] and Ankesha Guagusa (population 142,947) districts of Awi zone, Amhara regional state, north-western Ethiopia, which together include 38 kebeles (smallest administrative units) and 10 health centres. These two districts were chosen in collaboration with the NTD department of the Federal Ministry of Health due to the lack of other DMDI programmes in the area and the co-endemicity of LF, podoconiosis and leprosy, with an estimated combined prevalence of 1% [7].
Study design
Using the Medical Research Council (MRC) Complex Intervention Framework, to develop, pilot, evaluate and implement the intervention, we conducted a pre-post study comparing physical and psychosocial characteristics of affected persons and community members at baseline and 6 months after initiation of the EnDPoINT care package.
Participants
People living with LF, podoconiosis and sequalae of leprosy in the (predominantly rural) target districts were identified from health records and were invited into the study by health extension workers (community health workers with 1 year of pre-service training). Inclusion criteria were: presence of lower limb lymphoedema (lower leg swelling) caused by one of the three diseases; age > 18 years; living in the district for more than 6 months; being willing to participate through written informed consent. Exclusion criteria were: presence of a terminal illness that prevented engagement in the care package; presence of nodules or wounds that required surgical or specialist management (those in the latter category were appropriately referred).
Community members in Guangua and Ankesha Guagusa districts were selected by allocating a sample proportional to the total population in each district and kebele, and selecting households within kebeles based on simple random sampling. We took samples from all Kebeles (sub-district) and got (villages) in the study districts. We selected samples randomly from each kebele/got proportional to population size. Inclusion criteria were resident of Guangua or Ankesha Guagusa districts ≥ 6 months; age > 18 years old; free of acute or debilitating illness; and able to communicate sufficiently in the local language.
Intervention
The EnDPoINT care package has been described elsewhere [15] and was delivered during Phase 3 between January and August 2021. In essence, the package included interventions at three levels of the health system (health organisation, facility, and community) to support limb care and mental health care appropriate to the three NTDs. At the healthcare organisation level, central coordination, supportive supervision and monitoring were introduced. At the facility level, primary care clinicians were trained in holistic management, offered simple hygiene supplies and given the skills to engage patients in self-care. At the community level, workshops were held to raise awareness and reduce stigma, community members were trained in DMDI and a Community Advisory Board was established.
Sample size calculations
For the patient cohort, the sample size calculation was based on results from EnDPoINT Phase 2 [16], with reduction in disability, as measured by the WHO Disability Assessment Schedule-2.0 (WHODAS-2.0), selected as the primary outcome measure. To detect a 3.1-point change in WHODAS-2.0 score, with 90% power at 5% significance, a one sample t-test of the paired differences requires 99 participants. With 13 health facilities in total, and assuming an intracluster correlation coefficient (ICC) of 0.05, the number of participants per facility needed for the analysis was 99*(1–0.05)/(13–99*0.05) = 12 per health facility, or a total of 156. Allowing for 20% attrition, the estimated total sample required was 195 participants. The community sample size calculation was based on an earlier knowledge, attitudes and practice (KAP) study in Ethiopia in which 55% of a community sample exhibited correct practice [20]. An unpaired before and after comparison would require 805 participants at each time point for 80% power at 5% significance to detect a change in correct practice from 55 to 62%. With a design effect of 1.2 the estimated sample size was 805*1.2 = 966.
Study outcomes
For affected persons, physical outcomes included: average maximum lower limb and foot circumferences in cm (measured at the widest point of the calf or foot and averaged across both legs); presence of wounds or nodules on either leg; report of ‘attacks’ of acute dermatolymphangitis in the last month (acute ‘attack’ being defined as the leg becoming hot, painful and more swollen); and signs of infection on either leg. The WHODAS-2.0, validated in Ethiopia, was used to assess disability. Scores range from 12 to 60, with higher scores reflecting greater disability [21]. Psychosocial outcomes for patients included: the Patient Health Questionnaire-9 (PHQ-9) to measure depressive symptoms [22], with total scores ranging from 0 (no depressive symptoms) to 27 (severe depressive symptoms); the Dermatology Life Quality Index (DLQI) validated in southern Ethiopia [23], with scores ranging from 0 (no effect of disease on life) to 30 (extremely large effect of disease on life); the Fast Alcohol Screening Test (FAST) to assess alcohol use disorder [24]; the discrimination section of the Discrimination and Stigma Scale (DISC)−12 [25], with modifications described in a previous Ethiopian study [26], scores ranging from 1 to 56, with higher scores reflecting more discrimination; the 11-item Internalized Stigma Related to Lymphoedema (ISRL) scale adapted from the Internalized Stigma of Mental Illness Inventory (ISMI) scale [27], scores ranging from 11 (less stigma) to 44 (more stigma); and the Oslo-3 Social Support Scale (OSSS) [28], with scores from 3 to 14, higher scores representing better support.
Amongst community members, outcomes included: access to sources of health information (five questions about frequency of exposure to sources such as magazines, radio, television, health education sessions and meetings, with total scores ranging between 5 and 15, and higher scores indicating better access to health information sources); knowledge about the causes of lymphoedema (ten indicators for podoconiosis, LF and leprosy with total scores ranging from 0 to 12, with higher scores representing better knowledge); attitudes towards persons affected by lymphoedema using an index constituting 13 negatively framed statements identified from previous reports [29, 30]; degree of closeness towards persons affected by lymphoedema using the 7-item Social Distance Scale (SDS) [31], adapted to the study context, with total scores ranging from 7 to 35 where lower scores indicated higher willingness to have social interactions.
For the cost-effectiveness analysis, data on use of healthcare services and associated costs were collected in relation to affected persons’ lymphoedema, hospitalisations, medication, traditional remedies and money borrowing over the past year. We also measured the number of days completely unable to work (or go to school), and the number of days when they experienced some difficulties when working (or attending school).
Statistical analysis
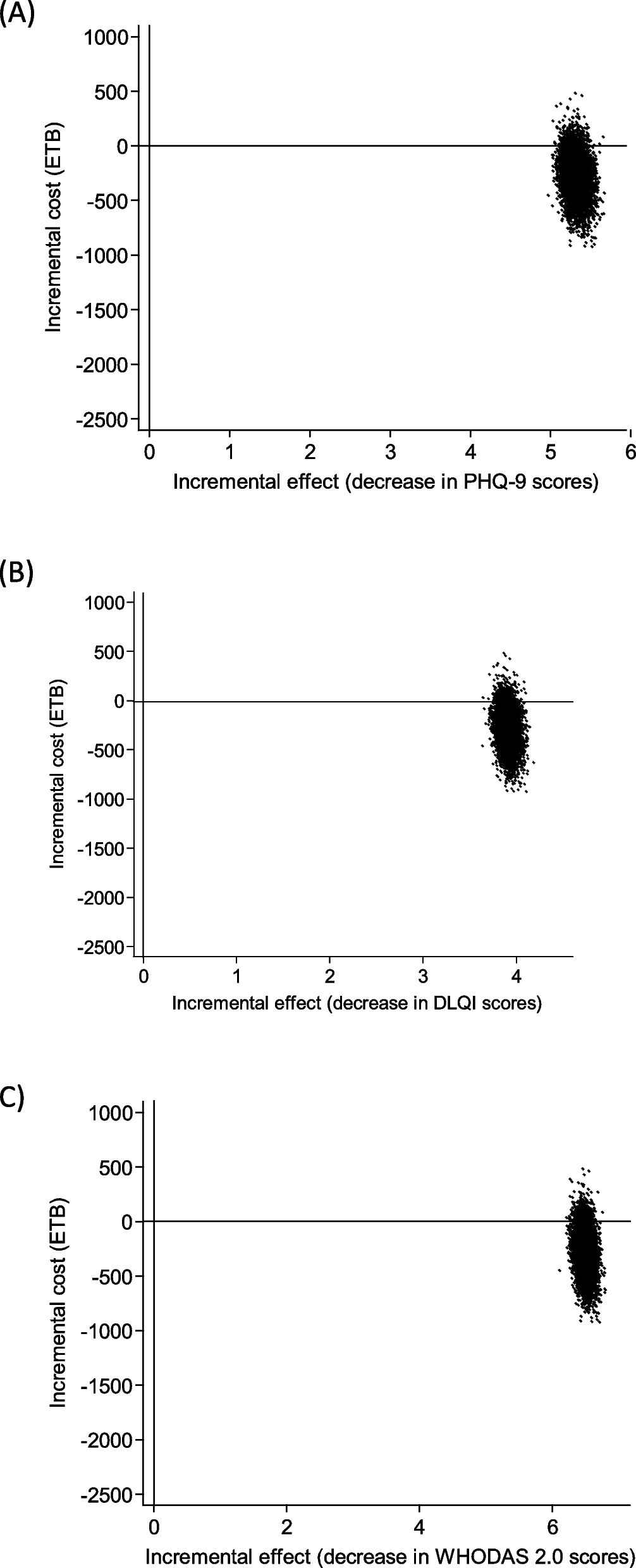
All data were collected by trained field staff and transferred to an Excel data sheet for cleaning and verification, before being imported to Stata version 17 (College station, TX 77845, USA) for analysis. Mixed effects linear regression models with a random effect for participant and fixed effect for time-point were used to assess the magnitude and direction of changes as well as the statistical significance of trends in outcomes between baseline and 6 months after initiation of the care package. All models were adjusted for district, sex, religion, occupation, marital status, and relative income category. Loss in work productivity was costed using the average daily wages (Poor Persons’ General consumer Price Index-Deflated Real Wages) for unskilled rural labour in Ethiopia, using figures for Amhara region in 2015 [32] and adjusting them to 2021 using purchasing power parity [33]. Costs in Ethiopian Birr (ETB) were converted to US dollars ($) using the average spot exchange rate [34] and to international dollars (I$) using purchasing power parity to reflect differences in price levels between countries [33]. Costs included cost of the EnDPoINT care package (estimated per patient in 2019 (870 ETB)[35] and adjusted to 2021 (1,028 ETB) [33] and cost of work productivity loss due to lymphoedema. For ethical reasons, we did not have a control group in this study, and all the participants were offered an intervention. In the cost-effectiveness analysis, we used the baseline data as control, or ‘usual care’. Effectiveness estimates for PHQ-9, DLQI and WHODAS-2.0 were adjusted using a mixed-effects regression model with patient ID as random effect. Covariates included in the model as fixed effects were: age, gender, educational attainment, occupation, relative income, employment, and time point of data collection (baseline or 6 months).
For the incremental cost-effectiveness ratio (ICER), the difference in costs between 6 months and baseline (incremental cost) was divided by the difference in effectiveness scores between 6 months and baseline (incremental effect). The denominator was multiplied by −1 to reflect the fact that lower effectiveness scores indicate a better outcome.
$$\text\frac_}} - \text_}} }}_}} - \text_}} } \right)* - 1}}$$
Ninety-five per cent confidence levels for incremental costs and incremental effectiveness outcomes were calculated using the non-parametric bootstrap method (5000 replications). Cost-effectiveness analysis was conducted in Stata 17 (StataCorp, 2021).
Role of the funding source
The views expressed in this publication are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care. The funders had no role in the study design; the collection, analysis, and interpretation of data; the writing of the report; or the decision to submit the paper for publication.

Comments (0)