
Remember me
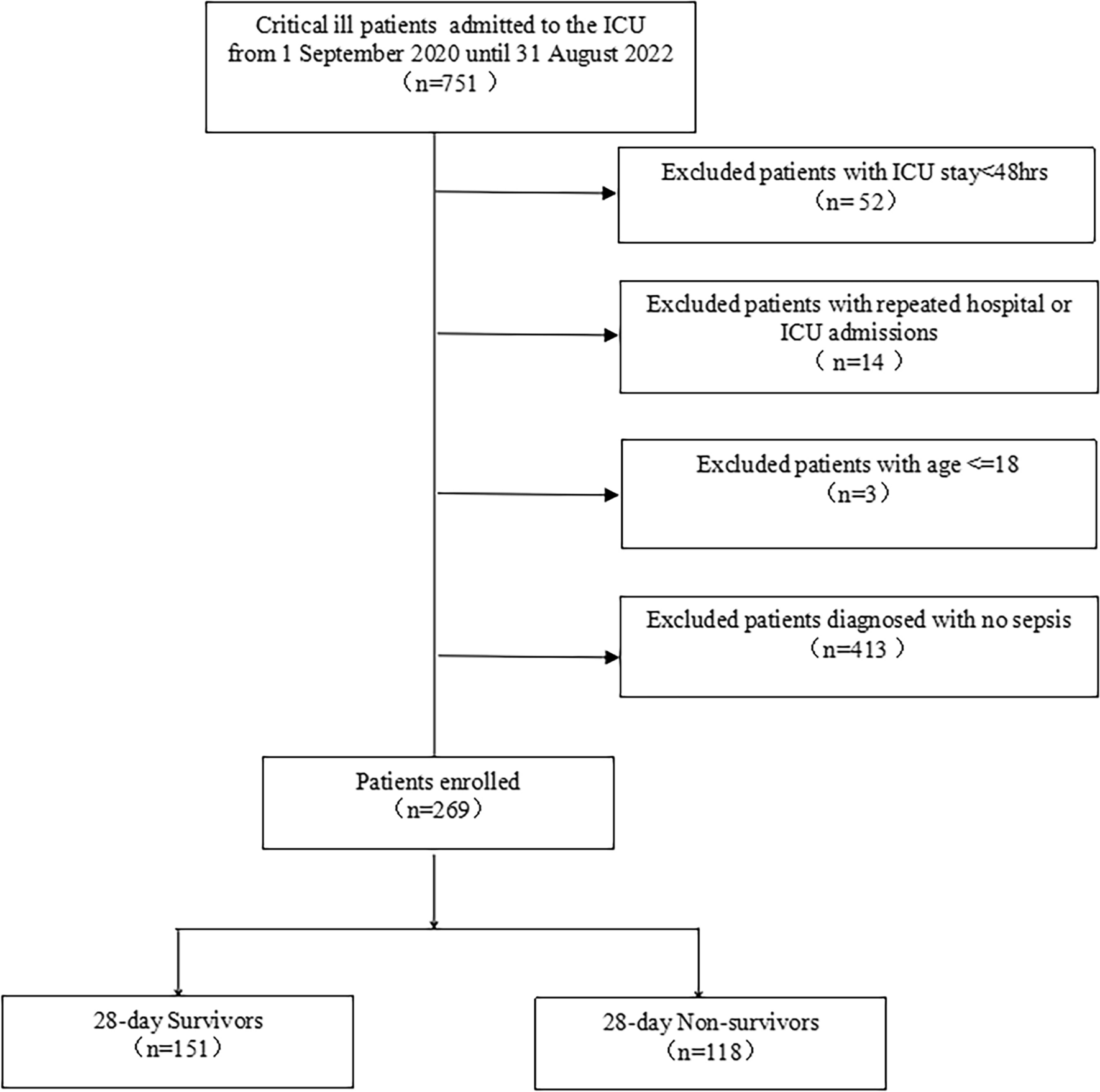
This study derives from an analysis of the “Cardiogenic Shock Registry Mannheim” (CARESMA-registry). The CARESMA-registry represents a prospective single-center registry including consecutive CS-patients who were admitted to the ICU for internal medicine of the University Medical Center Mannheim (UMM), Germany, from June 2019 to May 2021 (clinicaltrials.gov identifier: NCT05575856), as recently published [15]. Patients were eligible for inclusion when CS was the cause of admission for ICU. In detail, this included patients in the emergency department, outpatient clinic, and general ward, as well as patients in the diagnostic area, such as coronary angiography and computed tomography. Besides these, patients with onset of CS outside the hospital, were included. Furthermore, for this analysis solely patients with CS and documented PaCO2 and PaO2 on admission were included. In 35 patients no documentation of PaCO2 and PaO2 was available on admission. Therefore, these patients were excluded. No further exclusion criteria were applied. An overview of the inclusion process is illustrated in Supplemental Fig. 1.
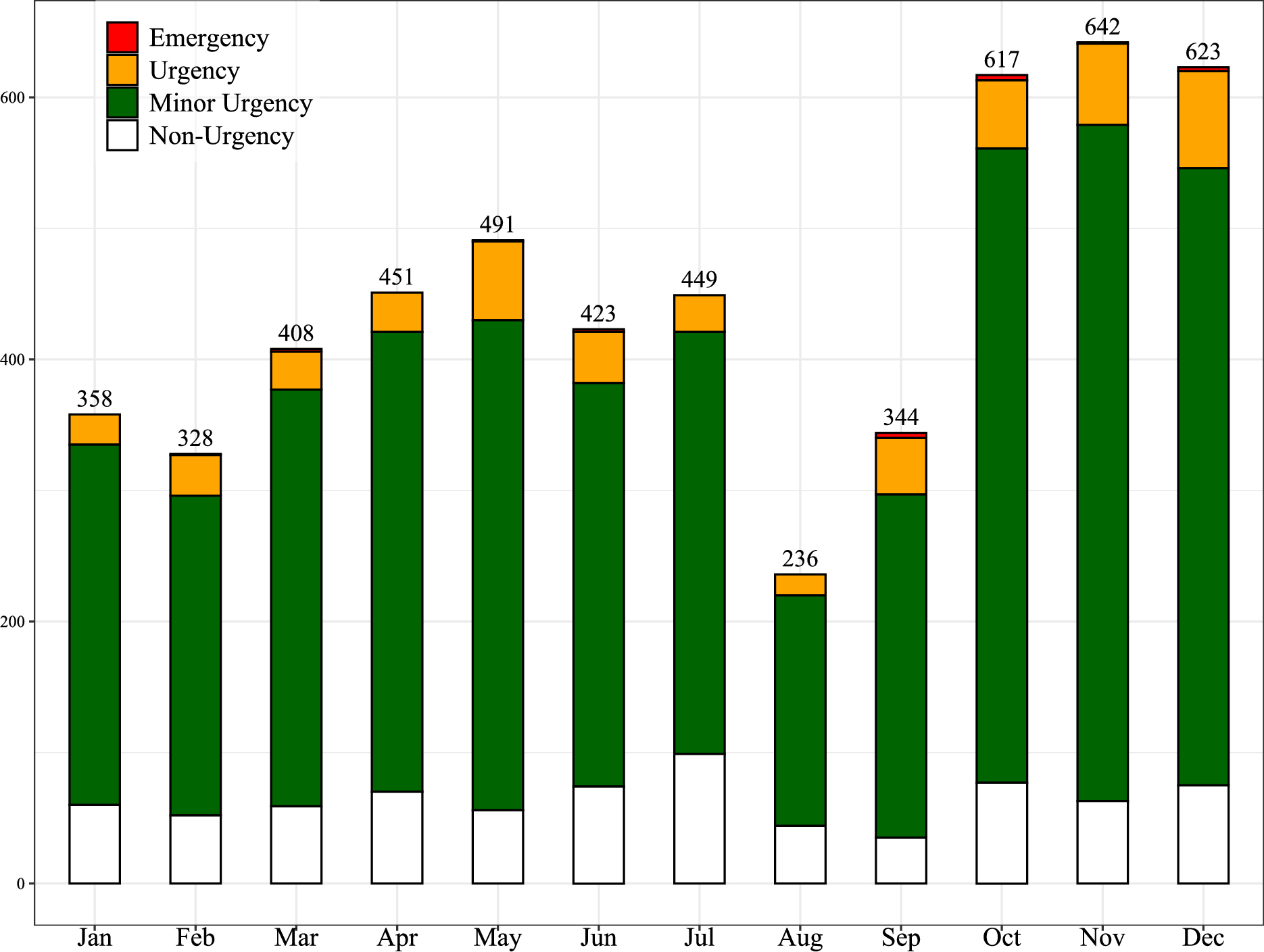
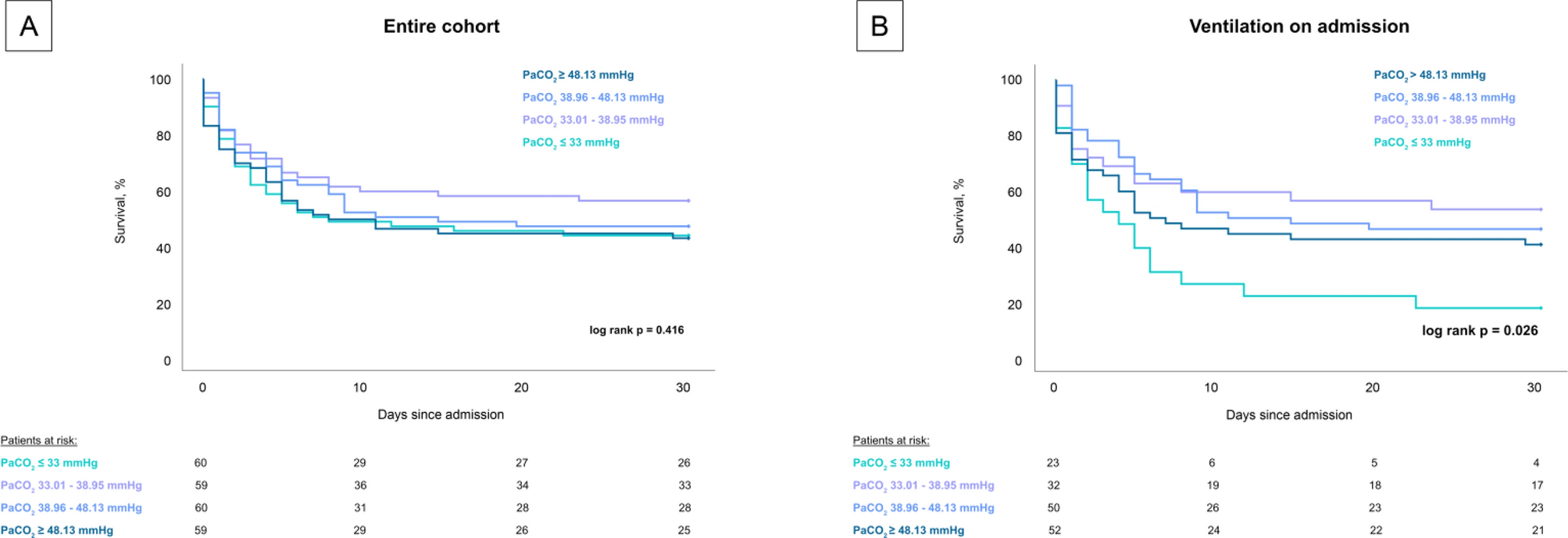
Fig. 1
Prognostic impact of PaCO2 startified by quartiles on 30-day all-cause mortality in the entire cohort (panel A) and the subgroup of ventilated patients (panel B)
Study endpointsThe primary endpoint was 30-day all-cause mortality. All-cause mortality was recorded using the electronic hospital information system and by directly contacting state resident registration offices (‘bureau of mortality statistics’). Identification of patients was verified by name, surname, day of birth, and registered living address. No patient was lost to follow-up with regard to all-cause mortality at 30 days.
The secondary endpoint of the study comprised the correlation of PaCO2 on admission with clinically relevant and laboratory parameters.
Definition of CSDiagnosis of CS was determined according to the recommendations of the Acute Cardiovascular Care Association of the European Society of Cardiology [16]. Accordingly, CS is defined by hypotension (systolic blood pressure < 90 mmHg) for more than 30 min despite adequate filling status or need for vasopressor or inotropic therapy to achieve systolic blood pressure > 90 mmHg. Additionally, signs for end-organ hypoperfusion must be present such as oliguria with urine output < 30 mL/hour, altered mental status, cold clammy skin, and increased lactate > 2 mmol/L. Moreover, patterns (increased left ventricular end diastolic pressure > 20 mmHg, elevated pulmonary capillary wedge pressure diagnosed by pulmonary artery catheterization or by mitral E-wave deceleration time ≤ 130 ms in echocardiography) or indirect signs (pulmonary congestion confirmed by clinical examination or chest X-ray) of elevated left ventricular filling pressures were mandatory for CS diagnosis. To finally confirm that CS was the fundamental cause of critical illness, a distinct cause of CS was required. This was not limited to acute myocardial infarction. Most recommendations are derived from studies of patients with infarct-related CS. However, data from these studies cannot be transferred to non-infarct-related CS [17, 18]. Therefore, this study included patients with various causes of CS such as arrhythmia, acute decompensated heat failure, pulmonary embolism, valvular heart disease, Tako-Tsubo-cardiomyopathy, pericardial tamponade, and aortic dissection. Cardiac tamponade and pulmonary embolism were classified as CS despite the obstructive mechanism of shock since existing recommendations and guidelines on acute heart failure and CS classify these entities as potential underlying causes for CS [19,20,21,22]. Aortic dissection was defined as CS when aortic valve regurgitation was the leading cause for hemodynamic instability [20]. Arrhythmic causes comprised supraventricular arrhythmias such as atrial fibrillation or flutter, atrial tachycardia as well as ventricular tachycardia including primarily ventricular fibrillation.
Data collectionAll relevant clinical data related to the index event were documented using the electronic hospital information system, organizing patient data, including admission documents, vital signs, laboratory values, treatment data and consult notes.
The presence of CS, as well as important laboratory data, ICU-related scores, hemodynamic measurements, ventilator parameters were assessed on the day of admission. Further data being documented contained baseline characteristics, prior medical history, length of index hospital stay, data derived from imaging diagnostics, as well as pharmacological therapies. Documentation of source data was performed by intensivists and ICU nurses during routine clinical care. All procedures were followed in accordance with the ethical standards of the medical ethics committee II of the Medical Faculty Mannheim, University of Heidelberg, Germany and with the Helsinki Declaration of 1964.
Respiratory parameters and intensive care related information were documented by the IntelliSpace Critical Care and anesthesia information system (ICCA, Philips, Philips GmbH Market DACH, Hamburg, Germany) implemented on the ICU and the connected respiratory machines. Furthermore, blood gas samples including PaO2 and PaCO2 were determined on admission for every patient. Respiratory settings were adjusted by the responsible medical team on the ward to achieve a PaO2 goal of > 65 mmHg and a PaCO2 that would maintain a pH > 7.20.
Statistical methodsQuantitative data is presented as median and interquartile range (IQR). They were compared using the Student’s t test for normally distributed data or the Mann–Whitney U test for nonparametric data. Deviations from a Gaussian distribution were tested by the Kolmogorov–Smirnov test. Qualitative data are presented as absolute and relative frequencies and were compared using the Chi-square test or the Fisher’s exact test, as appropriate. Kaplan–Meier analyses on 30-day survival according to the quartiles of PaCO2 and PaO2 were performed in the entire cohort and in the subgroup of ventilated CS-patients, patients with acute myocardial infarction and acute decompensated heart failure. Univariable hazard ratios (HR) were given together with 95% confidence intervals by performing Cox regression. Thereafter, multivariable Cox regression models were developed using the “backwards selection” option and variables with p-values < 0.10 in the univariable analyses. Furthermore, solely clinically relevant variables such as age, body mass index, sex, chronic obstructive pulmonary disease (COPD), bilirubin, creatinine, troponine I, pH value, norepinephrine dose, cardiac arrest, heart rate, SCAI CS stage, cause of CS, Acute Physiology score, SOFA score, peak inspiratory pressure, peak end-expiratory pressure (PEEP), driving pressure, tidal volume, respiratory rate, mechanical power, lung compliance, PaO2 ≥ 65 mmHg and PaO2/FiO2 on admission were eligible for the multivariable Cox regression model.
Results of all statistical tests were considered significant for p < 0.05. SPSS (Version 29, IBM, Armonk, New York) was used for statistics.
Comments (0)