
Remember me
A total of 34 patients with post-stroke dysphagia admitted to our clinic between April 2023 and October 2023 were included in this prospective, double-blind, randomized controlled study. The inclusion and exclusion criteria are presented in Table 1.
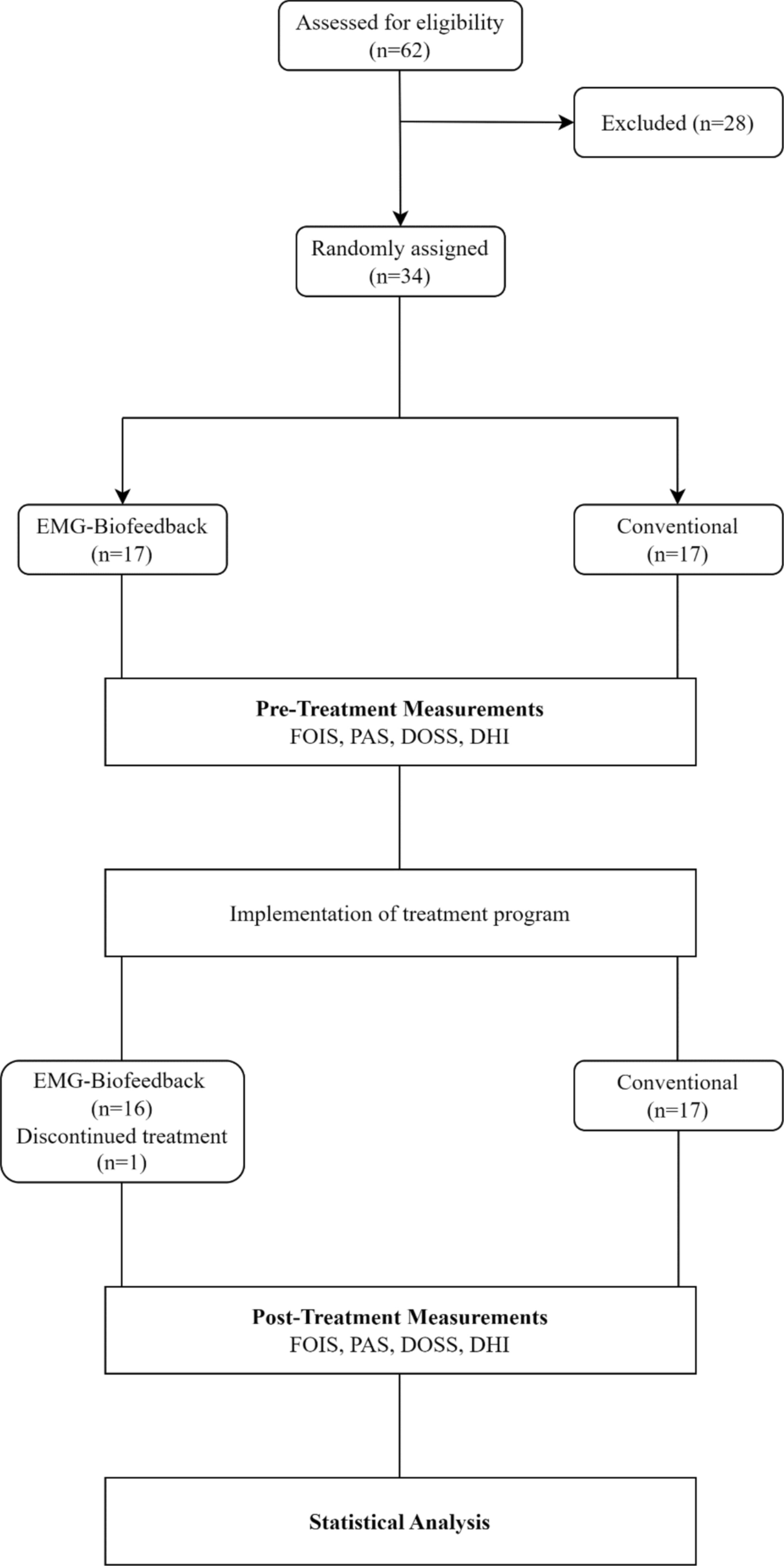
Table 1 Inclusion and exclusion criteria of the participantsPatients were randomized into two groups of 17 patients by simple random sampling method through a computer program: EMG-Biofeedback (study) and conventional therapy (control). Patients' demographic information, medical and family history, time elapsed after stroke, radiological findings, stroke type, lesion location, type of nutrition, medications used, and post-stroke treatments were recorded. Additionally, Mini-Mental State Examination (MMSE), Functional Ambulation Scale (FAS), Barthel Index, and Gugging Swallowing Screen (GUSS) scores were recorded. Functional Oral Intake Scale (FOIS), Penetration–Aspiration Scale (PAS), Dysphagia Outcome and Severity Scale (DOSS), and Dysphagia Handicap Index (DHI) were administered to the patients in both groups before and after therapy. Assessments were conducted by another researcher blinded to the intervention and unaware of which group the individuals belonged to, both before and after therapy. All data extracted were analyzed by a data analyst blinded to the study. Since one patient in the study group did not participate in the final evaluation, the data were analyzed based on a total of 33 patients, with 16 patients in the study group and 17 patients in the control group. Fig. 1 illustrates the flow diagram of the study design.
EthicsThe study was approved by the Institutional Review Board and conducted in accordance with the principles of the Declaration of Helsinki. The study protocol was approved by the Clinical Research Ethics Committee of the Faculty of Medicine at Kocaeli University with approval number “KAEK/02.bI.04”. Additionally, it was approved by the Turkish Medicines and Medical Devices Agency with approval number “E-68869993-000-1019202”. Every patient provided informed consent by signing the consent form. The study was registered on Clinicaltrials.gov with registration number “NCT05832658”.
Fig. 1
Flow diagram of the study. FOIS functional oral intake scale, PAS Penetration aspiration scale, DOSS Dysphagia outcome and severity scale, DHI Dysphagia handicap index
InterventionEffortful SwallowAll participants were taught the effortful swallow. They were instructed to push the hard palate strongly with their tongue, squeeze all the throat muscles, and swallow forcefully. To facilitate learning, the patients were told to "swallow hard, as if swallowing something stuck in your throat." The maneuver was practiced several times to ensure that the patients performed it correctly.
Mendelsohn ManeuverPatients’ laryngeal prominence (thyroid notch) was palpated, and the patients were asked to palpate it as well. Patients were instructed to place their index finger on the laryngeal prominence, swallow, and hold the laryngeal prominence in the highest position for 2–3 s without allowing it to drop. It was emphasized that breathing would stop during this time, and if they could breathe, they were doing it wrong. The patients were given several practice attempts to ensure proper execution of the exercise. During the treatment period, they were encouraged to hold the position for a longer duration, and for those able to do so, this duration was extended to 5 s.
Patients in the control group performed the Mendelsohn maneuver and the effortful swallow for 15 min each for a total of 30 min with only verbal feedback such as "hold longer" and "squeeze harder." The study group practiced these exercises with game-based EMG-biofeedback. The total duration of sessions for both groups was kept equal. Both groups received treatment for a total of 15 sessions over a period of 3 weeks, with sessions held 5 days a week.
Patients with sitting balance were seated on a chair. For patients unable to sit, their beds were adjusted to an upright position, and exercise therapy was commenced. Both groups were given 2 ml of liquid to moisten the oropharynx during exercises when needed, and for patients at risk of aspiration, the oral cavity was moistened with moist gauze. Short rest periods were provided for patients during exercise sessions.
Game-Based EMG-BiofeedbackPatients included in the study group performed effortful swallow and Mendelsohn maneuvers with game-based EMG-biofeedback. Game-based EMG-biofeedback was applied using the Vitalstim Plus device (Chattanooga Group, Hixson, TN, USA) and the Vitalstim Software obtained from the manufacturer's official website. Before electrode placement, the skin was prepared by cleaning with chlorhexidine/alcohol wipes. The bipolar surface electrode was placed horizontally over both sides of the patient's submental muscles (mylohyoid, geniohyoid, anterior digastric), equidistant from the midline, and the reference electrode was secured under the clavicle. sEMG was performed using a Vitalstim Plus device (Chattanooga Group, Hixson, TN, USA) with a selectable band-pass filter, a heart rate filter with a bandwidth of 100–370 Hz with the heart rate filter turned on, and a 50 Hz notch filter, with a root mean square (RMS) range of 0.2 to 2000 μV and a sensitivity of 0.1 μV RMS, and the measurements were simultaneously transferred via Bluetooth to the Vitalstim Software. EMG-biofeedback was applied with the rose game and bunny game available in the Vitalstim Software program on the computer screen. The games provided patients with both visual and auditory feedback (Fig. 2).
Fig. 2
"Effortful swallow" was performed with the rose game and "Mendelsohn maneuver" was performed with the rabbit game. In the effortful swallow, the patients were asked to press their tongue hard against their palate and swallow with all their strength. Meanwhile, the rose on the screen would fade when the patients exceeded a threshold in muscle activity. Once the patient completely faded the rose, indicating the completion of the swallowing activity, they would relax their muscles, and the rose would bloom again, completing one exercise cycle. The game provided not only visual but also auditory feedback at certain stages. In the rabbit game, the patient was visualized as a rabbit climbing a hill, reaching the top where a carrot awaited. Patients performed the Mendelsohn maneuver by attempting to elevate the larynx for 2–3 s to reach the highest point. As the patient exceeded the threshold value of muscle activity, the bunny in the game would climb the hill and reach the top. Then, during the relaxation phase, the patient would release themselves, and the bunny would descend the hill and eat the carrot, completing one exercise cycle. The relaxation period was set to 2 s, and if muscle relaxation was not achieved within 2 s, the game would reset. This approach not only focused on strength but also involved coordination-based tasks. The duration of holding the larynx at the highest point could reach up to a maximum of 5 s, depending on the individual and the treatment process. Like the rose game, the rabbit game provided both visual and auditory feedback.
To successfully complete each cycle in both games, the patient's muscle activity had to exceed the predetermined threshold value. The exercise duration for each game was 15 min. The threshold value was determined based on the average amplitude of three swallows measured through the Vitalstim Software, and a value above the average was set. Thresholds in the games were initially set as low as possible to build patients' confidence in their swallowing abilities and increase their motivation. The thresholds were gradually increased over time based on the patient's performance, aiming to achieve higher levels of muscle activity (Fig. 3).
Fig. 3 Evaluation MeasurementsFunctional Oral Intake Scale (FOIS)
Evaluation MeasurementsFunctional Oral Intake Scale (FOIS)FOIS was developed by Crary et al. [12] in 2005. It is a two-part scale with a total of 7 levels, indicating the functional oral intake of patients with dysphagia. It is used to determine whether an individual is dependent on tube feeding and to assess the level of oral intake. Items 1 to 3 assess the inability to feed orally, while items 4 to 7 assess the status of oral feeding. It has been evaluated as a suitable tool to determine the change in functional oral intake, particularly in stroke patients. Level 1 represents the worst level, while level 7 indicates the best level.
Penetration Aspiration Scale (PAS)PAS is an eight-item scale developed by Rosenbek et al. [13] in 1996 that provides information about the presence and severity of penetration and aspiration following instrumental videofluoroscopic swallowing assessment. The scale quantitatively determines the presence of penetration and aspiration, making it a reliable and highly clinically applicable tool for all consistencies. Scores are based primarily on the position of the food in the airway and whether it is expelled from the airway. A score of "1" indicates no penetration or aspiration, scores "2–3–4–5" indicate the presence of penetration, while scores "6–7–8" indicate the presence of aspiration.
Dysphagia Outcome Severity Scale (DOSS)DOSS was developed by O'Neil et al. [14] in 1999. Following videofluoroscopic swallowing evaluation, patients are assessed on a 7-point scale, ranging from normal (7) to severe (1). The scale allows for the classification of dysphagia outcome severity as normal (7), minimal (6), mild (5), mild/moderate (4), moderate (3), moderate/severe (2), and severe (1).
Dysphagia Handicap Index (DHI)DHI is one of the scales used to assess quality of life. Developed by Silbergleit et al. [18], DHI is a 25-item questionnaire that evaluates swallowing difficulty from three aspects: functional, physiological, and emotional. The questionnaire is completed through an interview between the clinician and the patient or their caregiver. Its Turkish validity and reliability were established by Çiyiltepe et al. [19]. Each question has three response options: "never," "sometimes," and "always." "Never" is scored as 0, "sometimes" as 2, and "always" as 4. Scores range from 0 to 100, with higher scores indicating poorer quality of life.
Statistical AnalysisStatistical evaluation was performed using IBM SPSS 20.0 (IBM Corp., Armonk, NY, USA). Conformity of the variables to normal distribution was examined by Shapiro–Wilk test. Normally distributed variables were expressed as mean ± standard deviation, and non-normally distributed variables were expressed as median (25th-75th percentile). Categorical variables were presented as frequency (percentage). The difference between the groups was determined by independent samples t-test and Mann–Whitney U test. Wilcoxon signed rank test was used for dependent group comparisons. The relationships between categorical variables were determined by Chi-square analysis. A p value of < 0.05 was considered statistically significant in all analyses.
Comments (0)