
Remember me
A descriptive longitudinal study was carried out on 127 adult post-COVID-19 patients who failed OD screening at discharge from the main university isolation hospital from July 2021 to March 2022. According to the isolation hospital policy, all patients were admitted with severe or critical illness. Severe illness was defined as individuals who had an oxygen saturation measured by pulse oximetry (SpO2) ≤ 94% on room air, a ratio of partial pressure of arterial oxygen to fraction of inspired oxygen (PaO2/FiO2) < 300 mmHg, marked tachypnea with respiratory frequency > 30 breaths/min, or lung infiltrates > 50%. Critical illness was defined as individuals who had acute respiratory failure, septic shock, and/or multiple organ dysfunctions [18]. Patients with severe illness received either conventional oxygen therapy (COT) or noninvasive ventilation (NIV), while patients with critical illness received either NIV or invasive mechanical ventilation (IMV). Patients under the age of eighteen and older than sixty-five, stroke patients, patients with previous OD, patients who have had OD because of neurological diseases or head and neck malignancies, and those with tracheostomies were excluded from the study. All participants provided written informed consent before the study.
MethodsAll participants underwent the following assessment protocol at the time of discharge from the hospital:
(A) Patient history:
- Demographic information (name, age, and gender).
- Medical history: including history of previous OD, neurological disorders such as stroke, or head and neck cancer. COVID-19 infection was established in the admitted patients by detecting SARS-CoV-2 RNA employing reverse transcription-polymerase chain reaction (RT-PCR). Patients with respiratory clinical syndrome consistent with acute infection were included in the study.
- Present history: including length of hospital stay, ageusia, anosmia, and dysphonia, as well as duration and method of delivery of oxygen therapy (Conventional oxygen therapy, non-invasive ventilation (NIV), and IMV).
(B) Clinical examination: this involves evaluating the patient's respiratory status by measuring heart rate, respiratory rate, and oxygen saturation using pulse oximetry.
(C) Screening for OD with the Arabic version of the "Eating Assessment Tool" (EAT-10)” [19] and the evidence-based "Yale swallow protocol" [15].
- The Arabic version of the "Eating Assessment Tool" (EAT-10)” is a self-administered questionnaire designed to assess OD in the Arabic-speaking population in a subjective manner. There are ten statements total, each given a 5-point rating on a scale from 0 (indicates no problem) to 4 (indicates severe problem). A summated EAT-10 total score falls between 0 and 40; a score of ≥ 3 indicates dysphagia. One's self-perception of dysphagia is higher when their EAT-10 score is elevated.
- The "Yale swallow protocol" (bedside swallowing assessment) involved three items:
I. Brief cognitive screen.
II. Oral mechanism examination.
III. The patient had a 3-oz water swallow test, the results of which were evaluated based on the following standards:
"PASS": Drinking 90 ml (3 oz) of water entirely and continuously without exhibiting overt aspiration signs, such as coughing or choking, during or right after the task.
"FAIL": The patient stopped/started swallowing before finishing the whole 3 oz or showed overt aspiration signs, such as coughing or choking, during or right after the task.
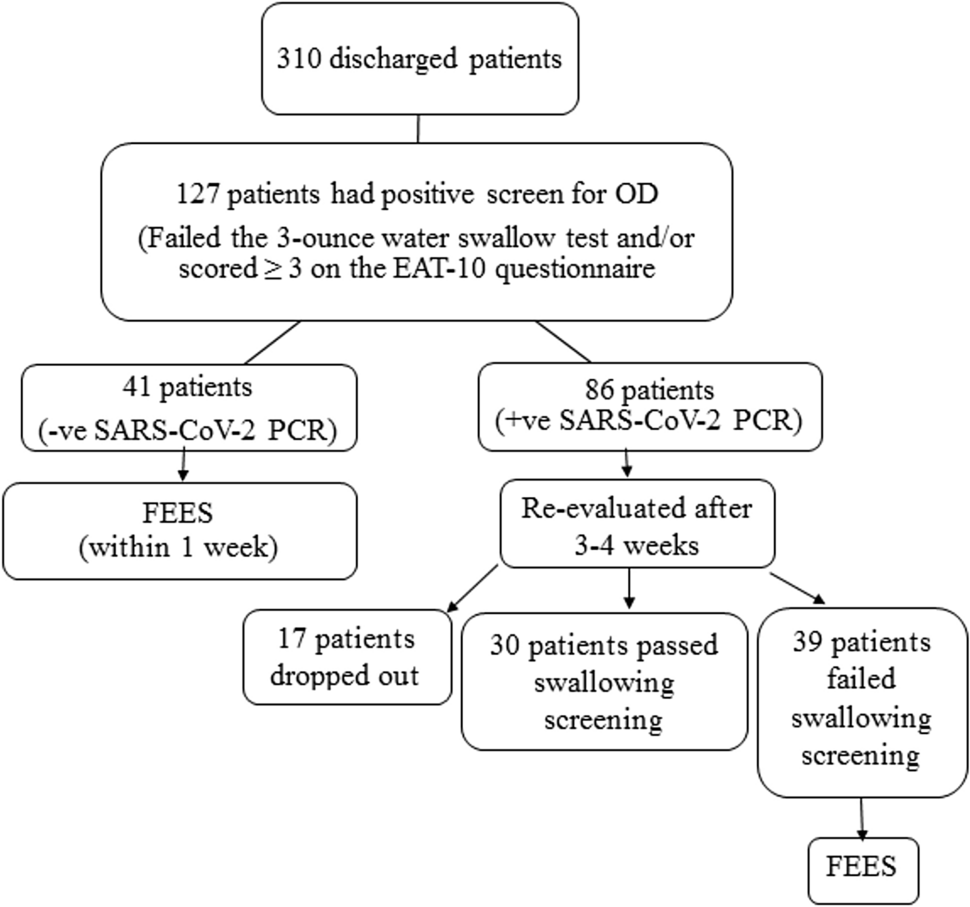
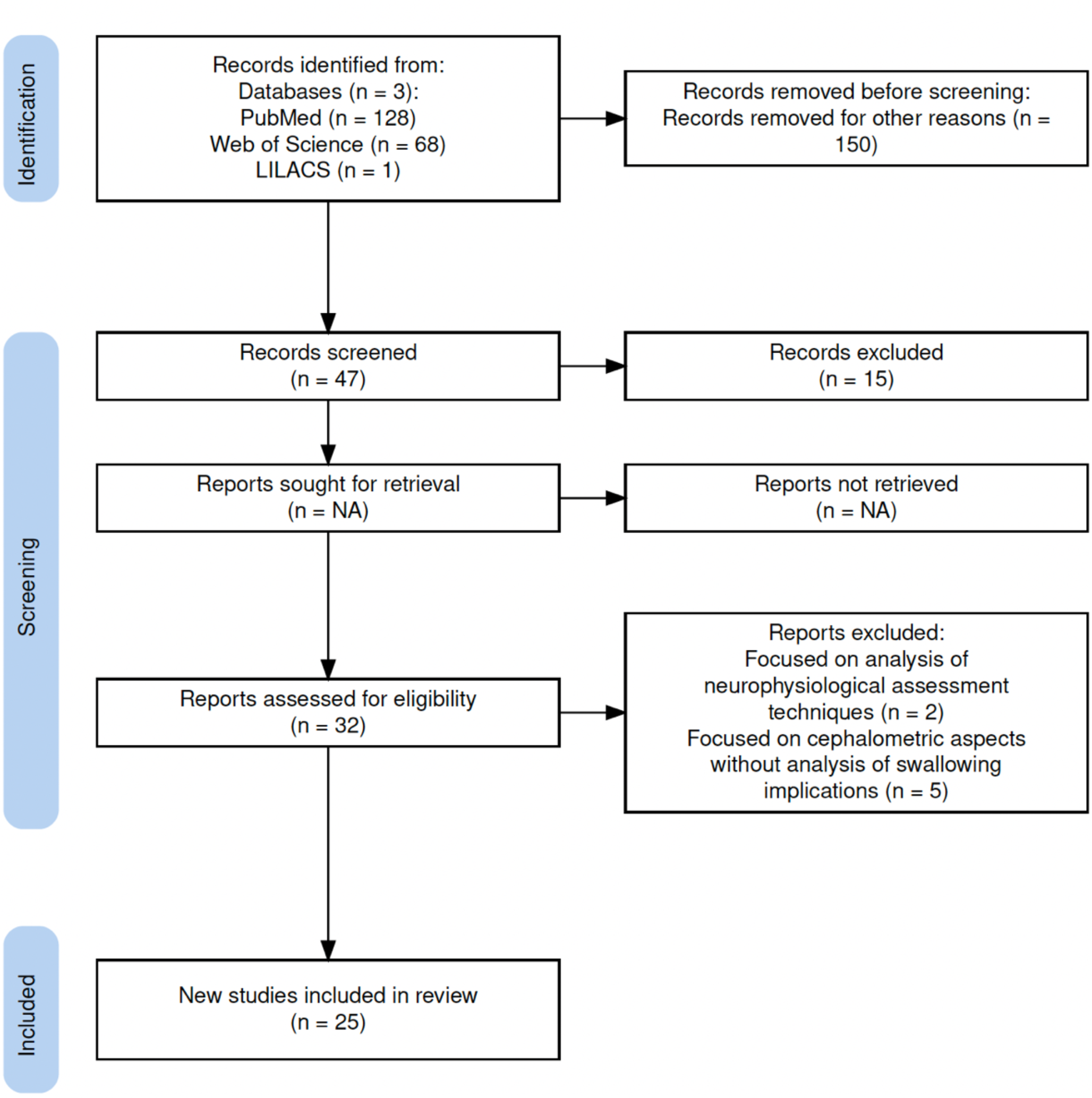
Adequate precautions were taken during the bedside swallowing assessment to avoid transmission of infection to the clinician. The phoniatrician was positioned at the patient's side, maintaining a distance of about 2 m [20]. Patients who had a positive screen for OD (failed the 3-oz water swallow test and/or scored ≥ 3 on the EAT-10 questionnaire) were included in the study. These were 127 patients out of 310 discharged patients who were screened for OD during the study period. The timing of fiberoptic endoscopic evaluation of swallowing (FEES) was determined according to the result of SARS-CoV-2 PCR at the time of discharge based on infection control measures and the potential persistence of viral RNA. Patients with negative SARS-CoV-2 PCR were evaluated by FEES within one week after discharge (Group 1 patients). For patients who had positive SARS-CoV-2 PCR, FEES was postponed, and compensatory treatment strategies (including bolus modification and postural techniques) or nasogastric tube feeding were considered till the 1st follow-up visit at 3–4 weeks after discharge when patients were reevaluated by screening tools at post-COVID-19 clinic in the university hospital. Patients who still failed OD screening were evaluated by FEES (Group 2 patients). Counting from the onset of COVID-19 symptoms, group 1 patients were considered in the early stage of recovery, and group 2 patients were considered in the late stage of recovery. The number of patients who underwent FEES was 80 (41 in group 1 and 39 in group 2) (Fig. 1).
Fig. 1
Flowchart of patient enrollment/exclusions and assessments
(D) Instrumental swallowing assessment:
- It was performed through fiberoptic endoscopic evaluation of swallowing (FEES). FEES was done using fiberoptic nasendoscopy “Henke-Sass-Wolf, type10” linked to a Lemke video camera (MC204) and software for recording and retrieving recorded materials. Personal protective equipment was used during the FEES.
- FEES Examination protocol [21] was used:
Part 1: Anatomic- physiologic assessment:
A. Visualization of pharynx and larynx at rest:
B. Secretions and how they were handled:
- The quantity, location, and reaction of the patient to secretions were noted over 2 min.
- The Murray secretion scale (MSS) [22], a four-grade scale, was used to rate the pooling of secretions in the hypopharynx and larynx before the first swallow. A patient was given score "1" when no visible or just a few bubbles of secretion were observed in the vallecula and hypopharynx, score "2" for deeply pooled secretions in the vallecula and pyriform sinus, score "4" when secretions were found in the laryngeal vestibule, and score "3" for any secretion that altered from a “2” to a “4” rating during the examination.
- Ice chip protocol was considered if secretions were observed in the laryngeal vestibule and the patient could not swallow saliva successfully.
C. Laryngeal function during both respiration and phonation.
D. Sensory testing:
- Laryngeal sensation was examined using the touch method, which involved touching the arytenoid cartilages by the tip of the flexible laryngoscope. The laryngeal sensation was considered to be grossly intact if any of the following signs were observed: laryngeal adductor reflex (LAR), a cough, a gag, eye blinking, tearing, throat clearing, swallowing, or a patient’s report of feeling the touch [23].
Part 2: Swallowing food and liquid:
During FEES, boluses with varying volumes and consistencies tinted green using a coloring agent were used: fluids (3 ml, 5 ml, 10 ml, and cup drinking), puree food (10 ml yogurt), and solid food (half biscuit) with two trials for each consistency. The patient's clinical status and swallowing function were considered when selecting the appropriate boluses. If aspiration occurred twice with any bolus amount or consistency and compensatory strategies failed to eliminate aspiration, these boluses were deemed unsafe for the patient.
- Swallowing function during FEES was assessed using two standard rating scales from video recordings: The penetration-aspiration scale (PAS) [24] and the Mansoura fiberoptic endoscopic evaluation of swallowing residue rating scale (MFRRS) [25]. The PAS is an eight-point rating scale that considers the material's depth into the airway and its clearance from the airway during swallowing trials. MFRRS is an accurate, anatomically based tool that is highly reliable for judging post-swallow pharyngeal residue during FEES. Two 7-point ordinal scales are used in MFRRS (one for pyriform sinus residue and one for vallecular residue).
Part 3: Therapeutic interventions:
Compensatory interventions were combined with "part 2" and trialed as soon as applicable. These included postural techniques, bolus modifications, and behavioral adjustments (e.g., washing down residue with liquid).
Statistical analysisIBM SPSS software, version 22.0, was used to input and analyze data. Numbers and percentages were used to describe the qualitative data. Quantitative data were characterized using the median (minimum and maximum) for non-parametric data and the mean and standard deviation for parametric data. Acquired results were deemed significant at the (0.05) level. The Chi-Square test was employed to compare two or more groups. For parametric tests, two independent groups were compared using the student t-test; for non-parametric tests, two independent groups were compared using the Mann–Whitney U test. The study employed stepwise logistic regression analysis to forecast independent variables associated with a binary outcome. In the univariate analysis, significant predictors were entered.
Comments (0)