The adaptation of 5C scale
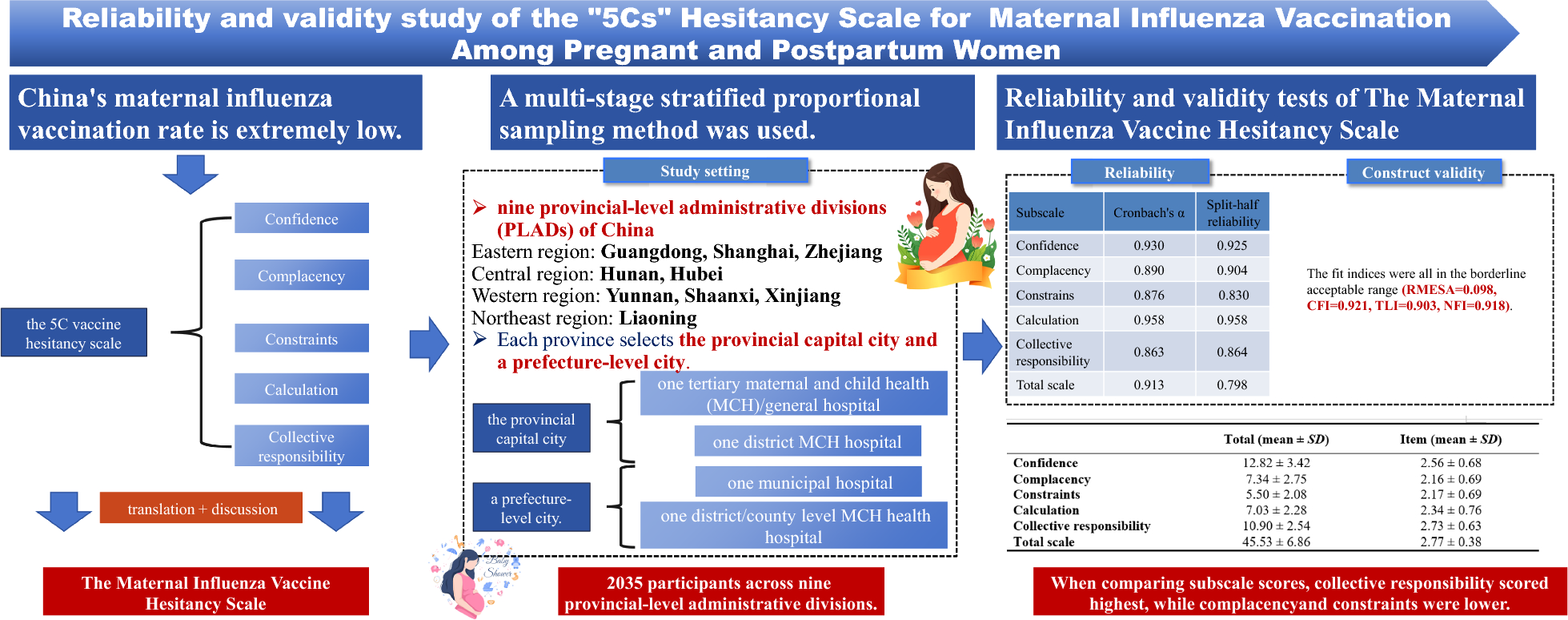
The Maternal Influenza Vaccine Hesitancy Scale was developed by Betsch et al. based on the 5C scale assessing influenza vaccination hesitancy among the general population in 2018. The original 5C scale included 15 items with five subscales: confidence (three items), complacency (three items), constraints (three items), calculative (three items), collective responsibility (three items). When adapted for usage in maternal influenza vaccine hesitancy, the structure of the scale remains unchanged, containing the same five subscales. We added “influenza” before vaccine/vaccination and the specific time “during pregnancy/postpartum” in each item. Furthermore, items related to the safety and effectiveness of fetuses/babies’ health were added in each confidence, complacency and collective responsibility subscale. In the confidence subscale, two additional items were added: (a)“ I am completely confident that influenza vaccination during pregnancy/postpartum is safe for the fetus/baby with breastfeeding.”, (b)“ Influenza vaccination during pregnancy/postpartum is effective for the fetus/baby with breastfeeding.”. In the complacency subscale, one additional item was added: “The fetus/baby’s immune system is so strong; it protects them against influenza.”. In the collective responsibility subscale, one additional item was added: “Getting the influenza vaccination during pregnancy/postpartum is important because it helps protect the fetus/baby.” As a result, a total of 19 items were established for the Maternal Influenza Vaccine Hesitancy Scale (Table 2).
Table 1 Individual characteristics of pregnant and postpartum women (n = 2035)Prior to the survey, the initial translation was completed by a native Chinese researcher, FYZ. Two senior experts, HJ and XQ, with more than 20 years of research experience in maternal and child health care evaluated and revised translation to ensure the accuracy and cultural appropriateness.
Study setting
From 17 January 2024 to 14 March 2024, the survey, using multi-stage stratified proportional sampling method, was conducted in nine provincial-level administrative divisions (PLADs) of China, including Guangdong, Zhejiang and Shanghai, representing eastern China; Hunan and Hubei, representing central China; Yunnan, Shaanxi and Xinjiang, representing western China; and Liaoning representing northeastern areas in China. The sample size in each PLAD was allocated based on its proportion of the total deliveries in the nine PLADs in 2022. In each PLAD, four sites were selected, one tertiary maternal and child health (MCH)/general hospital and one district MCH hospital in the provincial capital, as well as one municipal hospital and one district/county level MCH hospital in a prefecture city. The sample size in each city was allocated based on the proportion of deliveries in the city relative to the total number of deliveries in the PLAD in 2022. Furthermore, the sample size of each medical institution in the same city was allocated based on the ratio of delivery numbers of the two institutions in 2022.
Participants and data collection
We recruited pregnant women and postpartum women who scheduled antenatal health examinations during the survey period. The inclusion criteria included: (1) the participants were aged 18 and above; (2) the participants were either pregnant or within four months postpartum, and (3) the participants were able to understand and fill in the questionnaire by themselves.
The research has obtained the ethical approval of School of Public Health, Fudan University (IRB#2023-12-1093). During the survey, the trained staff invited eligible pregnant and postpartum women to participate in the survey and provided participants with the electronic QR code of a self-administered questionnaire via Wenjuanxing (www.wjx.cn), a widely used online questionnaire survey platform. Pregnant women invited to participate in the anonymous survey were required to scan the QR code via a mobile phone or other digital devices. At the beginning of the survey, an online informed consent process was set with a brief introduction, including the aim and contents of the online questionnaire and the estimated time of completion (7.18–32.60 min). All Participants provided informed consents. They could decide whether to continue or withdraw from the survey at any time during the survey. The online questionnaire included sociodemographic characteristics of participants and the Maternal Influenza Vaccine Hesitancy Scale, etc.
Quality control measures are as follows: (1) One quality control question was included in the questionnaire. If a respondent answered this question incorrectly, the questionnaire was considered invalid. (2) Pilot survey was conducted before the launch of the study, and it took at least 5 minutes to complete. Any questionnaire submitted in less than 3 minutes was deemed invalid.; (3) Questionnaires containing the same answer for every question were treated as invalid.
Questionnaires and measurementsSocio-demographic characteristics
During the survey, we collected the following socio-demographic information from the participants: age, perinatal stage, ethnic group, residence, educational level, annual household income, marital status, family structure, breastfeeding intention for pregnant women or breastfeeding status for postpartum women, parity.
The maternal influenza vaccine hesitancy scale
The Maternal Influenza Vaccine Hesitancy Scale consists of 5 items in the confidence subscale, 4 items in both the complacency and collective responsibility subscales, 3 items in the constraints and calculation subscale, with 19 items in total. The 4-point Likert scale, with scores ranging from 1 (Strongly disagree) to 4 (Strongly agree) was used for each item. High levels of confidence and collective responsibility indicated low levels of vaccine hesitancy [22]. High levels of complacency, constraints and calculation represented high levels of vaccine hesitancy [21, 22]. Therefore, items were reversely coded for the 4-point Likert in the complacency, constraints and calculation subscale. A mean score of items under each subscale was computed. Higher scores in each subscale indicated that pregnant women had higher confidence in the influenza vaccine, lower complacency about the risks of influenza, fewer constraints in accessing influenza vaccination, a more calculative approach to gathering influenza vaccine-related information, and a stronger sense of collective responsibility to protect others through influenza vaccination.
Data analysisReliability
The online questionnaire results were exported and sorted in Microsoft Excel 16.0 (Microsoft Corporation, Redmond, USA), and analyzed by SPSS 25.0 (IBM Corporation, Chicago, USA). Reliability analysis included internal consistency reliability and split-half reliability. We used Cronbach’s α coefficient to evaluate the internal consistency reliability and the Spearman-Brown coefficient to evaluate the split-half reliability between odd questions and even questions. A reliability coefficient above 0.7 was acceptable for the whole scale [23].
Validity
Validity was analyzed using construct validity. AMOS 23.0 (IBM Corporation, Chicago, USA) was used to analyze the construct validity. The construct validity of the questionnaire was evaluated by confirmatory factor analysis (CFA). Maximum likelihood estimation was used in CFA analysis. The good model fit for CFA was defined as: (1) root mean square error of approximation (RMSEA) < 0.1; (2) normed fit index (NFI) > 0.9; (3) comparative fit index (CFI) > 0.9; (4) Tucker-Lewis index(TLI) > 0.9[24].






Comments (0)