Functional Magnetic Resonance ImagingMechanism
Developed in 1990, functional magnetic resonance imaging (fMRI) quickly became popular for its ability to assess neuronal activity, aiding in pre-surgical planning, evaluating treatment responses, and offering a new tool to further the understanding of neuronal pathways [5, 6]. The rationale underlying this technique is the change in hemodynamic parameters in the brain which occurs as a metabolic response to increased neuronal activity; i.e. the quantification of changes in neurovascular coupling in response to specific conditions or tasks [7]. Two primary MRI techniques are used to detect response in hemodynamic activity of the brain: arterial spin labeling (ASL) and blood-oxygen-level-dependent (BOLD) contrast. In ASL, arterial blood water is magnetically labeled using radiofrequency pulses, allowing changes in local cerebral blood flow (CBF) to be quantified by measuring the difference in signal between labeled and unlabeled regions of the brain. Because of relatively poor signal-to-noise ratio and longer acquisition time resulting in low temporal resolution, ASL is now primarily utilized to quantify cerebral perfusion in patients with stroke, brain tumors and neurodegenerative conditions [8]. For the indication of functional neuroimaging, ASL has been largely supplanted by the BOLD technique. Rather than relying on magnetically labeled water molecules, BOLD indirectly detects changes in deoxygenated hemoglobin, which is paramagnetic and can be detected by MRI. When neurons are active and their consumption of oxygen increases, a compensatory increase in CBF to the active area of the brain lowers the concentration of deoxygenated hemoglobin and heightens the MR signal detected by BOLD fMRI [9]. The higher signal-to-noise ratio of BOLD, temporal resolution approaching physiologic neural activity (1–2 s) and wide availability and standardization of acquisition protocols have made this technique the gold standard for detecting changes in neurovascular coupling in the brain [10].
Healthy Bladder Control
Since the development of BOLD fMRI, hundreds of studies have utilized this technique to explore cortical and subcortical control of the LUT. This body of work has revolutionized our understanding of the brain-bladder interaction, confirming previously suspected brain regions involved in LUT control and identifying new ones. While there is significant variability in experimental conditions across these studies, the results have been surprisingly consistent overall. Based on these findings, Griffiths et al. have proposed a framework to summarize cortical bladder control by identifying three neural circuits that are involved in afferent communication with the LUT: Circuit one governs sensation and cognitive decision-making, primarily regulated by the thalamus, insula, PAG, and the prefrontal cortex. Circuit two involves the dorsal anterior cingulate cortex (ACC) and supplementary motor area (SMA). The ACC, often referred to as the limbic motor cortex, collaborates with the SMA to respond to bladder expansion and facilitate contractions of the pelvic floor and sphincter muscles to prevent unintentional loss of urine. Circuit three is responsible for the unconscious monitoring of bladder filling during low-volume states, with its function primarily managed by the PAG and parahippocampal regions of the temporal cortex. While the circuits are described individually for clarity, their functions are highly interconnected, and their mutual coordination is critical for effective bladder control [3].
Most studies utilizing BOLD fMRI to study brain function associated with lower urinary tract (LUT) control, including those utilized by Griffiths et al. to develop their bladder control framework, have focused on urinary storage [3, 11, 12]. However, several groups have successfully assessed brain activity associated with bladder voiding, both in healthy individuals and those with neurological conditions [11, 13,14,15]. Significant cortical activation compared to baseline was detected in all the studies examining healthy individuals. Areas with notable BOLD signal changes included many regions whose functions have been well-established in LUT control: the brainstem and midbrain (likely responsible for triggering and activating the mechanical aspects of the voiding response), the prefrontal cortex (responsible for the executive decision to initiate voiding), the insula, thalamus, and basal ganglia (providing sensory feedback during the process of voiding), as well as the primary motor cortex and the cingulate gyrus (likely regulating motor activity of the somatic and autonomic components of the LUT during voiding). These regions show consistent activation between sexes and appear to be engaged during voiding, independently of specific experimental setups.
Neurogenic Lower Urinary Tract Dysfunction
fMRI has been used to assess differences in cortical control of the LUT in patients with a variety of neurological conditions. When assessing these studies, it is important to differentiate not only the phase of micturition (storage or voiding), but also the comparison baseline (self or healthy controls). Finally, because involuntary bladder contractions (i.e., detrusor overactivity) are a common clinical correlate of NLUTD, whether voiding occurred as a result of a volitional or involuntary contraction is another important factor to take into account.
Multiple Sclerosis
The most significant body of literature on fMRI in NLUTD comes from the Khavari group at Houston Methodist, who have focused on female voiders and non-voiders with multiple sclerosis. They have carried out multiple studies focusing on neural activity during bladder filling and voiding. In one study that examined voiding initiation, they found that healthy individuals exhibited higher, more widespread activation compared to patients with multiple sclerosis [16]. Although the study did not differentiate between volitional and involuntary contractions, it suggested that LUT dysfunction in patients with multiple sclerosis is associated with markedly diminished brain activity.
Spinal Cord Injury
In a study of 8 patients with incomplete spinal cord injury, Zempleni et al. examined BOLD activation during bladder filling and re-assessed it after patients underwent a course of pudendal nerve stimulation [17]. They found that activation of several regions was increased following stimulation, further lending support to the idea that diminished activation of brain regions associated with LUT control is characteristic of NLUTD. To explore this idea, our group examined brain activity associated with involuntary (detrusor overactivity) bladder contractions in patients with complete spinal cord injuries (unpublished data). Compared to rest, some cortical activity was detected during both bladder filling preceding the contraction and during the contraction itself. However, there was no change in the neurosignature between filling and voiding that would be characteristic of a cortical micturition switch, i.e. the activation of regions expected to be involved in voiding (see Healthy Bladder Control above) was absent.
Stroke
Our group has utilized fMRI to assess bladder-associated brain activity in stroke survivors during voiding. In our initial study that did not differentiate volitional and involuntary contractions, we found diminished cortical activity in stroke patients compared to healthy controls during voiding [18]. In a follow up study, we compared detrusor overactivity to volitional contractions [19]. Consistent with others’ results, we found markedly diminished activation during detrusor overactivity contractions compared to volitional contractions in stroke survivors and in healthy individuals. Regions that have been previously shown by others to be active during voiding (midbrain, basal ganglia, insula, prefrontal cortex, motor cortex, cingulate cortex) were found to be active during volitional contractions in both stroke survivors and healthy participants, but not during involuntary contractions. These results suggest that a certain level of cortical activity and coordination is necessary to execute a volitional contraction, whereas detrusor overactivity contractions likely result from subcortical reflex processes.
Advantages and Limitations
FMRI is noninvasive and does not expose patients to ionizing radiation. Technological advancements, such as the development of more powerful magnets (e.g., 7 Tesla), have significantly improved its spatial resolution and signal to noise ratio. Additionally, innovations like faster imaging sequences have enhanced its temporal resolution to some extent [20]. As a result, it has revolutionized our understanding of brain-bladder control. However, fMRI also has several important shortcomings. Due to the intrinsic delay of the hemodynamic response, the temporal resolution of this technique remains in the range of seconds, which is much slower than the millisecond timescale of neuronal firing. Moreover, MRI requires significant capital and infrastructure investment, limiting its availability to larger centers, especially in the research setting. Finally, fMRI scans are typically acquired with participants in the supine position, which can be an important confounder for physiological tasks like bladder voiding [20]. Nonetheless, in the last two decades, fMRI has become the gold standard for evaluating bladder-related brain activity in states of health and disease. In the remainder of this review, we will examine other imaging modalities that have been utilized for this purpose and address their advantages and disadvantages with respect to fMRI.
Positron Emission TomographyMechanism
Developed in the 1970s, positron emission tomography (PET) relies on radiographic detection of an intravenously injected radioactive tracer [21]. A variety of tracers have been developed, each with a specialized application. However, for functional neuroimaging studies, 18-fluorodeoxyglucose (FDG) is utilized most commonly. FDG accumulates in tissues that metabolize glucose faster than surrounding tissue, such as active brain regions. The tracer then releases radiation that is detected by the scanner as two-dimensional images [22]. Cumulatively, multiple two-dimensional image planes detected by the scanner are used to generate a three-dimensional image and snapshot of FDG-avid tissues, such as active brain nuclei.
Healthy Bladder Control
In 1997, Blok et al. was the first to use PET to find active brain centers during micturition in healthy patients and demonstrated the presence of the pontine micturition center in humans [23]. This study and Nour et al. 2000 explored brain activation at similar stages of the cycle: at rest, during simulated voiding with saline, and when holding saline [23, 24]. Together, they set the ground for Griffith’s work to characterize the three neural circuits mentioned above [3]. During voiding, activation of the bilateral postcentral gyri, right insular cortex, and left thalamus indicated involvement of sensory processing in micturition control. Activation in the left ACC also implicated the limbic system’s role in micturition. Frontal gyrus, globus pallidus, and PAG activity demonstrated that voiding involves a decision-making process requiring coordination with subcortical brain regions. These foundational findings have since been confirmed via fMRI and other neuroimaging studies with greater depth and resolution.
Neurogenic Lower Urinary Tract Dysfunction
Although PET was the first hemodynamic/metabolic modality used to assess bladder-related brain activity, it has largely been supplanted by fMRI for reasons discussed below. However, two studies did use PET to characterize changes in brain activity in patients with NLUTD. The overarching purpose of these studies was to explore the effect of neuromodulation on bladder-related brain activity. Nevertheless, they offer valuable insights into how brain control of the LUT changes in patients with neurological conditions.
Kitta et al. demonstrated that compared to healthy controls, patients with Parkinson’s disease exhibited diminished pontine and ACC activity during bladder filling associated with detrusor overactivity [25]. Meanwhile, areas commonly found to have diminished activation in other NLUTD-associated conditions exhibited no difference between the healthy and PD group. This suggests that despite etiology-based variation in brain activation, LUTS are caused by attenuated brain activation along the three circuits outlined by Griffith et al.
In another study utilizing PET, Herzog et al. assessed changes in brain activity in patients with Parkinson’s disease after they underwent deep brain stimulation (DBS) electrode implantation into the subthalamic nucleus [26]. In contrast with Kitta et al.’s study, an increase in cystometric bladder capacity and reduction in urinary urgency was interestingly accompanied by a decrease in ACC and prefrontal cortex activation [25, 26].
While activation/deactivation patterns noted by these authors in response to neuromodulation are not necessarily consistent with the hypothesis that NLUTD is associated with global brain activity reduction, all of the changes occurred in regions known to be involved in LUT control, suggesting that aberrant activity of these areas leads to NLUTD in the first place.
Advantages and Limitations
PET has a spatial resolution of 4–10 mm and a relatively low temporal resolution on the order of seconds to minutes. In 2003, Feng et al. demonstrated that PET based measurement of regional CBF was on par to that of ASL fMRI, an fMRI technique not commonly used for functional neuroimaging today (see fMRI section above) [27]. Other limitations in utilizing PET for neuroimaging in NLUTD are rooted in its mechanism. Mainly, the tracers emit radiation, limiting studies requiring consecutive imaging and posing potential health risks for patients. While consecutive imaging has been performed, such as in Nour et al. 2000, both the diminished spatiotemporal resolution, radiation aspects and the requirements to prepare the tracer for each imaging study on have relegated PET to being a rarely-used imaging modality [24].
Functional Near-Infrared SpectroscopyMechanism
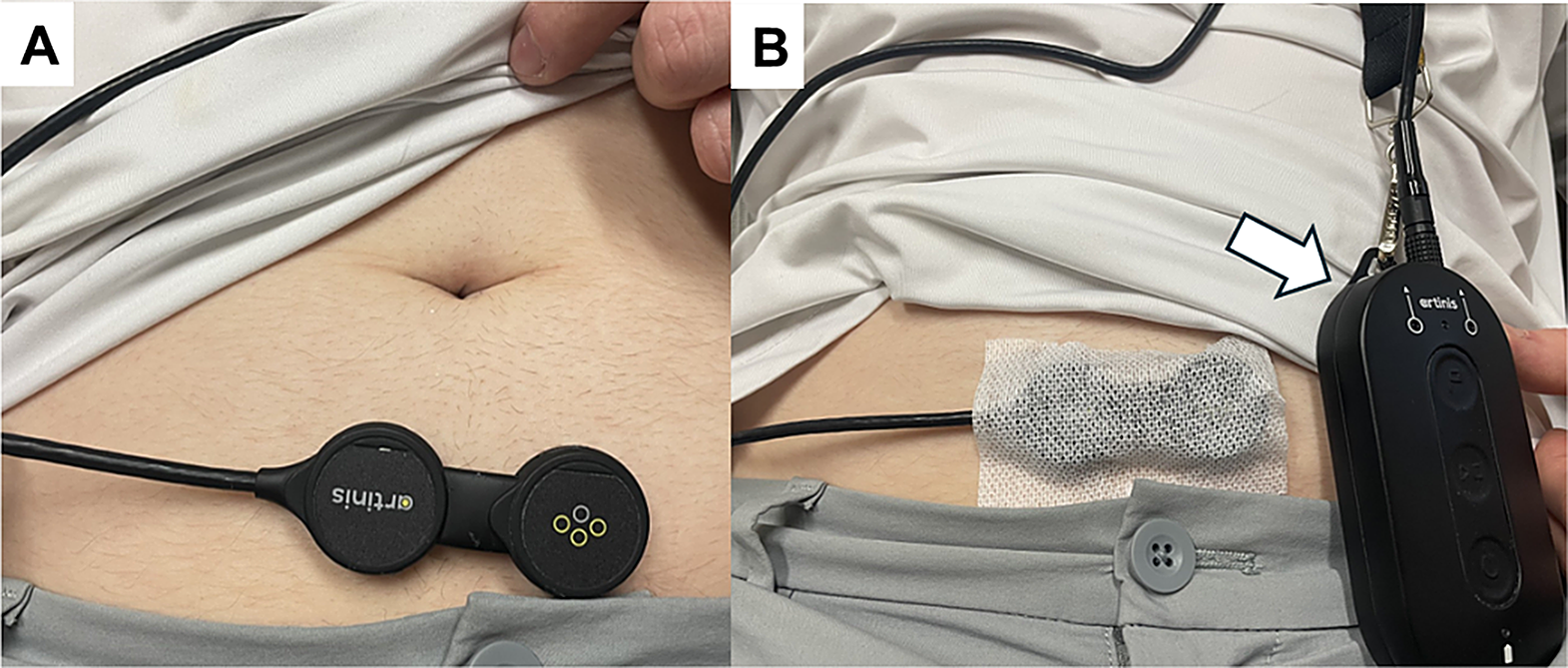
Functional near-infrared spectroscopy (fNIRS) has emerged as a promising functional neuroimaging technique that utilizes light waves to detect levels of oxygenated and deoxygenated hemoglobin in the cortex. The fNIRS cap contains probes that emit specific wavelength photons that penetrate the skin, subcutaneous tissue, skull and the other investing layers of the brain to a depth of 5–8 mm. Absorption of these photons by tissue generates dispersed light waves with varying intensities based on the oxygenation status of the tissue. As a result, oxygen consumption in the cortex can be indirectly assessed allowing one to make inferences about cortical activity at that location [28].
Applications in Neurogenic Lower Urinary Tract Dysfunction
Sakakibara et al. used fNIRS to compare brain activity between healthy individuals and patients with neurogenic detrusor overactivity secondary to various underlying neurological conditions [29]. Continuous measurements via fNIRS were taken during bladder filling and voiding. They found that compared to healthy controls, prefrontal brain activity was diminished in patients with NLUTD during bladder filling. Furthermore, while there were changes in prefrontal cortex oxygenation during the transition between storage and voiding in healthy individuals, detrusor overactivity contractions in NLUTD patients were not accompanied by significant changes in prefrontal hemodynamics. In two follow-up studies, the same group investigated the effect of anticholinergic therapy on fNIRS readings in patients with neurogenic detrusor overactivity, finding that prefrontal oxygenation increased during bladder filling after anticholinergic treatment [30, 31]. In both studies, changes in prefrontal fNIRS activity correlated with reductions in incontinence and other clinical parameters. Taken together, these findings align with those obtained using fMRI and PET, suggesting that reduced bladder-related brain activity is characteristic of NLUTD [29,30,31].
Advantages and Limitations
Unlike MRI, fNIRS recordings can be obtained in a standard clinical setting thanks to the portability of NIRS equipment. This portability not only dramatically lowers costs but also allows data acquisition in sitting or standing positions, mimicking physiological postures during micturition. In addition, fNIRS offers about a 10-fold improvement in temporal resolution compared to fMRI, enabling the capture of rapid changes in brain activity. These advantages are offset by several drawbacks of fNIRS. First, the spatial resolution of fNIRS is relatively poor compared to fMRI, making it less precise in pinpointing exact areas of brain activation. Secondly, fNIRS is limited by depth of penetration, with imaging generally confined to the cortical surface. Furthermore, fNIRS signals can be influenced by scalp blood flow and are susceptible to motion artifacts, which can complicate data interpretation [32]. Despite these limitations, fNIRS has found a niche in neuroimaging for LUT conditions due to its noninvasive, portable nature and ability to record brain activity in more naturalistic settings.
Functional UltrasonographyMechanism
Similarly to other hemodynamic-based neuroimaging modalities, functional ultrasound (fUS) measures blood flow, acting as a proxy for neurovascular activation. In concept, fUS is similar to a conventional Doppler ultrasound. By emitting a focused beam, a Doppler ultrasound provides a small column of a two-dimensional image based on the reflected echoes. In contrast, fUS relies on the release of plane or two-dimensional waves, which can cover an entire cross-section of an object with fewer ultrasound pulses. Due to its speed, it provides a lower spatial resolution per individual image. However, when these plane waves are released at different angles simultaneously at the same target, fUS can interpret and combine the echoes into a compound image with high spatial resolution. With an acquisition rate of approximately 50 compound images per 100ms, fUS also has high temporal resolution. Additionally, echo frequency distinguishes blood flow from other tissues, allowing for blood volume change quantification and correlation with neurovascular coupling [33]. With a spatial resolution on the order of 100 microns and temporal resolution approaching 0.01 s, this technology is emerging as an exciting modality for functional neuroimaging.
Applications in LUT Function
At present, noise generated by bony structures that enclose the target of interest (e.g., skull in the case of the brain) limits the application of this modality to animal models and intraoperative settings. However, fUS offers important advantages compared to fMRI as the gold standard. In addition to improved temporal resolution, fUS can be used to image small neural structures, such as the spinal cord, that are notoriously difficult to assess using fMRI. In a pilot study of patients undergoing implantation of a spinal cord stimulator for pain, Agyeman et al. examined the response of the thoracic spinal cord to bladder filling and emptying [34]. The authors performed urodynamics in a series of anesthetized able-bodied patients finding a strong correlation between the hemodynamic signal obtained in the dorsal spinal cord and bladder pressure. The same group employed fUS to study spinal cord activity in rats undergoing bladder filling and spontaneous emptying. Based on the strong correlation between spinal cord response and LUT activity, the authors developed a computational model able to predict LUT events based on hemodynamic signal derived from the spinal cord [35].
Advantages and Limitations
As above, fUS is currently limited to invasive monitoring by its signal-to-noise ratio. However, innovations in image acquisition will eventually make this modality noninvasive. For example, low-frequency probes (1–3 MHz) used in transcranial Doppler ultrasound can image intracerebral segments of the basilar arteries through the temporal bone window– the thinnest part of the skull [36]. Lower frequencies enhance bone penetration and reduce signal attenuation and scattering, although, they decrease spatial resolution due to longer wavelengths. Nonetheless, using low-frequency probes in fUS could enable noninvasive imaging.
Another innovation that may compensate for bone attenuation without sacrificing spatial resolution is the use of intravenous microbubble contrast agents. These enable brain fUS in rats with intact skulls due to the large echo frequency difference between the microbubble gas and surrounding tissue [37]. Fast imaging is ideal for avoiding bursting microbubbles, which may reduce that echo frequency difference, making it well-suited for fUS. This method achieved a spatial resolution of 100 micrometers and a temporal resolution of 2 milliseconds, comparable to fUS conducted via a plastic skull window. Since microbubble contrast is already used in vascular and renal imaging, it could have similar potential for human neuroimaging applications. Further investigation into this non-invasive approach could increase the accessibility of fUS neuroimaging to outpatient settings.


Comments (0)