
Remember me

Male urinary incontinence (UI) is a common complication following radical prostatectomy (RP) for prostate cancer. Post-prostatectomy incontinence rates vary significantly, ranging from 4 to 69%, depending on symptom severity. Severe incontinence occurs in approximately 8% of patients’ post-prostatectomy [1,2,3].
Radiation therapy (RT) is frequently indicated in prostate cancer cases to control positive margins or extra-prostatic malignancy. Approximately 30–40% of men who are undergoing artificial urinary sphincter (AUS) had received prior RT [4]. RT can lead to significant periurethral tissue damage, fibrosis, reduced vascularity, and poor wound healing, which complicates subsequent surgical interventions for UI [5].
This review aims to comprehensively evaluate the surgical options for managing male UI following RT for prostate cancer, including implanting an AUS and a male urethral sling. By analysing current literature and clinical studies, this review seeks to provide insights into the optimal timing, outcomes, complications, and quality of life improvements associated with these surgical interventions.
Male Urethral SlingsMale urethral slings are a popular surgical option for managing post-prostatectomy UI. These devices improve continence by compressing and repositioning the posterior urethra. Non-adjustable retrourethral transobturator slings (RTS) are currently the most widely used type of male urethral sling. The RTS restores the urethra to a pre-prostatectomy position by relocating the proximal bulbar urethra cranially by 2 to 3 cm within the pelvis. The pelvic floor muscles create higher pressure in the pelvic outlet, supporting the urethra and preventing urine leakage during straining [6]. Chan et al. further demonstrated the ‘dynamic compression’ effect of the RTS on the urethra during coughing and Valsalva manoeuvres [7]. Both ‘direct’ and ‘dynamic” compression’ are purported to contribute to continence following a RTS procedure.
A meta-analysis by Ghaffar et al. evaluated the effectiveness of urethral slings in treating male stress urinary incontinence in patients with prior RT [8]. The analysis included 27 studies with over 2,500 participants and found that patients with a history of RT had significantly lower odds of success (OR 0.68) and cure (OR 0.67) compared to those without RT. This effect held true for both fixed and adjustable sling types. In their subgroup analysis of the type of slings, the AdVance™ subgroup (fixed transobturator sling) had lower odds of success (OR 0.66), and both the AdVance™ and ATOMS® (adjustable sling) subgroups had lower odds of cure (OR 0.59 and OR 0.70, respectively). Additionally, patients who had prior RT had about three times the odds of experiencing complications such as sling removal or infection compared to non-RT patients.
In patients with a history of RT, the American Urological Association (AUA) and the Society of Urodynamics, Female Pelvic Medicine & Urogenital Reconstruction (SUFU) recommend AUS over male urethral slings, citing a lack of good evidence for the efficacy of male urethral slings in this subgroup [9]. The European Association of Urology (EAU) guidelines also suggest that prior RT may negatively impact the outcome of non-adjustable male urethral sling surgery [10].
The lower success rate in patients with a history of RT may be attributed to several factors: direct sphincteric damage from RT, reduced compliance of urethral tissue impairing adequate compression by the sling, and radiation-induced periurethral fibrosis reducing urethral laxity [6, 8]. RT also increases the risk of bladder dysfunction, like detrusor overactivity, which could negatively impact the effectiveness of male urethral slings [11, 12].
Artificial Urinary SphinctersSince the 1970s, the AUS has been considered the gold standard treatment for post-prostatectomy urinary incontinence. The AUS (prototyped by AMS 800™) comprises three primary components: the cuff, the pump, and the reservoir. Only patients with adequate manual dexterity and cognition are considered suitable candidates for AUS, which carries specific risks of complications such as erosion (6–8%), infection (5–6%), and mechanical failure (6–23% over 7 to 13 years) [6].
AUS Implantation TechniqueThe standard technique for AUS implantation involves placing the cuff around the bulbar urethra through a perineal incision under general or spinal anaesthesia. Achieving haemostasis is critical to reduce the risk of postoperative hematoma and infection. Anatomical variations, previous surgeries, and patient-specific risk factors need to be considered to tailor the surgical approach effectively [4, 13].
The procedure begins with a midline perineal incision to expose the bulbar urethra. The bulbospongiosus muscle is carefully dissected to gain access to the urethra. The AUS cuff is then placed around the bulbar urethra, with the size of the cuff being crucial for effective functioning and minimizing the risk of erosion. The reservoir is typically placed in the space of Retzius, though some surgeons may choose a different location based on the patient’s anatomy and prior surgeries. The pump is positioned in the scrotum, requiring the creation of a small subdartos pouch to securely house it.
Robot-assisted laparoscopic AUS implantation has gained traction recently as an approach that offers several advantages, particularly in complex cases. It allows for precise dissection around the bladder neck and prostate, potentially reducing intraoperative and postoperative complications [14]. This could potentially reduce the risk of injury to the urethra in post-RT patients, where dissection is anticipated to be challenging. While studies on robot-assisted laparoscopic AUS implantation have shown high continence rates and low complication rates [14], specific data on post-RT patients is sparse. Its use case and economic viability is yet to be proven in large scale studies.
Pathophysiological Effect of RT on AUSRT causes significant tissue damage, posing considerable challenges for AUS implantation. Radiation-induced progressive obliterative endarteritis compromises the blood supply to the urethra, increasing the risk of cuff erosion and infection [15]. Bates et al. identified a history of pelvic RT as an independent risk factor for erosions following AUS placement, underscoring the impact of RT on vascular integrity and tissue health [4]. This vascular compromise also diminishes the urethral tissue’s resilience, making it more susceptible to complications such as infection and erosion.
A systematic review and meta-analysis by Zhang and Xu aimed to compare the incontinence rates and complications in patients receiving AUS with and without prior RT [16]. They included 18 studies, comprising both prospective and retrospective cohorts, that met the criteria of comparing outcomes of AUS implantation in patients with and without RT. The meta-analysis revealed that patients with a history of RT had significantly reduced odds of achieving complete continence after AUS placement, with an odds ratio (OR) of 0.35. Additionally, there was a statistically significant increased risk of revision surgery (OR: 1.74), erosions (OR: 2.00), and explantations (OR: 3.00) in the RT group. Although the risk of infections showed a non-significant increase (OR: 2.51), the results suggested a potential trend towards higher infection rates in RT patients. Interestingly, the study found no significant differences in the risk of urethral atrophy (OR: 1.18) and mechanical failure (OR: 0.90) between the RT and non-RT groups. The authors however attributed this possibly to the small number of studies and small sample sizes that reported on urethral atrophy [16]. We will discuss these issues in detail in subsequent sections.
Timing of AUS PlacementSeveral studies have examined the outcomes of placing an AUS before or after RT, especially in the context of prostate cancer treatment.
A retrospective analysis confirmed that RT could be safely administered after AUS placement without increasing the risk of complications like infection or device erosion. This study included 306 patients treated from 1987 to 2016 and found no significant differences in adverse event rates between those who had RT before versus after AUS implantation [17].
Another retrospective review of 194 patients compared the outcomes of AUS placement before and after RT [18]. The post-AUS RT group, had significantly higher continence rates (p = 0.029) and no incidences of device erosion or infection within 180 days follow-up. On the other hand, the pre-AUS RT group, which had a higher 9.7% rate of both erosion and infection, but differences were not statistically significant. Similarly, the pre-AUS RT group had a higher frequency of revision surgeries. These findings suggest that undergoing RT after AUS placement may lead to better continence outcomes with similar complication rates. The preserved tissue integrity and vascularity before RT are possibly factors that could contribute to these improved outcomes.
Management of RT Stricture Prior to AUS ImplantationThe management of RT induced urethral strictures before AUS implantation is critical for ensuring the long-term success of incontinence treatment. Buccal mucosa graft urethroplasty (BMGU) maybe a suitable option to address these strictures. This technique involves using a buccal mucosa graft to substitute and augment a strictured segment of the urethra, providing a robust urethral bed that could withstand an AUS implantation.
A prospective database analysis performed by Maurer et al. in 2019 reported about 17 patients who underwent AUS implantation after BMGU. The median follow-up was 24 months [19]. A majority (76.5%) of these patients received pelvic RT, with the rates of objective, subjective, and social continence being 70.6%, 88.2%, and 94.1%, respectively. Although there was a higher risk of infection in patients with a history of BMGU compared to those without (11.8% vs. 2.7%), the explantation-free survival rate was not significantly different. These findings suggest that BMGU was an effective procedure for patients with radiation-induced urethral strictures who were eventually planned for AUS implantation.
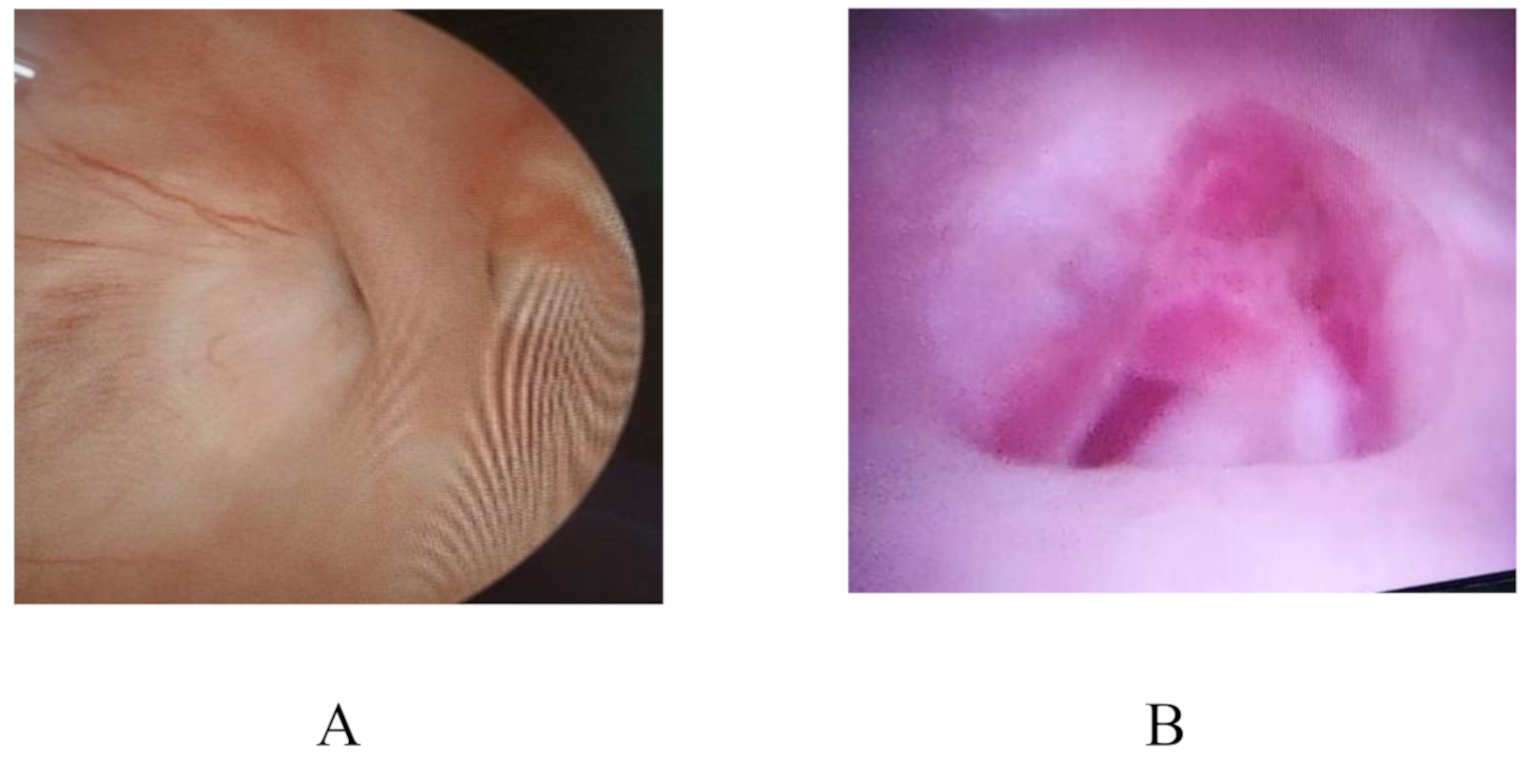
Management of Urethral ErosionErosion and infection are significant complications following AUS implantation, particularly in patients with prior RT. A recent retrospective study reported that the majority of patients with AUS cuff erosion (66%) exhibited scrotal inflammatory changes, characterized by tenderness, erythema, and swelling. A smaller proportion (43%) experienced obstructive voiding symptoms and 34% experienced worsening incontinence [20]. Figure 1 shows an example of urethral erosion seen at the time of surgery.
Zhang & Xu in their meta-analysis of several studies have showed an increased risk of urethral erosion in AUS implantations post-RT [16].
Urethroscopy can be used to detect early signs of impending urethral erosion, which could appear as mucosal hyperaemia or thinning. Some authors have described temporarily deactivating the AUS for 6–8 weeks to prevent further damage [5], but its utility to salvage the AUS is not proven. Once erosion occurs and the eroded cuff breaches the urethral mucosa, it has to be assumed that there would be corresponding infection of the entire AUS system [5].
Management of erosion typically involves explantation of the eroded device to allow tissue healing before considering re-implantation. This healing period can range from several months to a year, depending on the extent of tissue damage. Infections are typically managed by explantation of the device and administration of antibiotics, followed by re-implantation after a period of coalescence.
While most authors do not distinguish specifically between erosion and infection, there has been reports of being able to replace the sphincteric cuff in cases of uninfected ‘sterile erosion’ [21]. Evidence of this has however been scarce.
More recently, Shumaker et al. reported that delayed explantation or no explantation were viable options, especially in patients that were surgically unfit [22]. The authors postulated that in cases of subacute erosion, a capsule might form around the urethral defect, potentially preventing local infection. However, they also stated such a phenomena is usually not evident during AUS explantation, where there is often no adherence of the cuff to a pseudocapsule or to the corpus spongiosum [22].
Fig. 1
Hemi-circumferential erosion seen on the ventral surface of the urethra
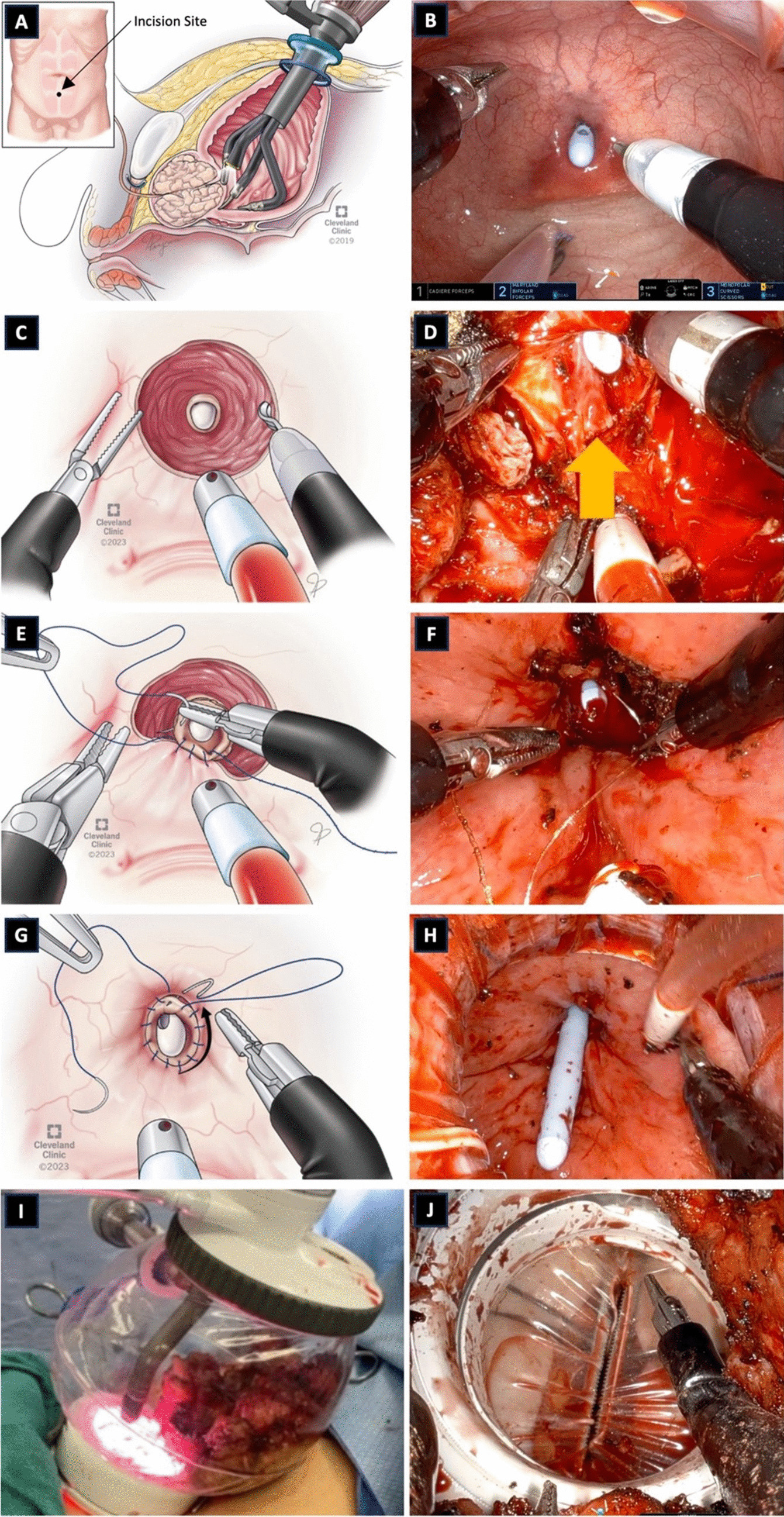
Fig. 2
Gull-wing TC modification with flap of tunica albuginea (green arrow) being harvested from the corpus cavernosum (CC) and being flapped onto the urethra (Ur) (direction depicted with blue arrow)
Management of Persistent UI after AUS ImplantationManaging persistent UI following AUS implantation in patients who have undergone RT requires a multifaceted approach. Radiation-induced changes, such as fibrosis and reduced vascularity in the urethra, bladder wall structure, and detrusor function [5], often necessitate tailored interventions. One key strategy is the thorough pre-operative assessment of urethral and bladder function. This includes urodynamic studies to evaluate bladder compliance, capacity, and detrusor overactivity.
In Zhang & Xu’s meta-analysis [16], patients with a history of RT exhibited a statistically significant 65% lower likelihood of successful outcomes with AUS implantation and experienced some degree of persistent UI after surgery. This was similar to the rates reported by Bates et al. in their meta-analysis of 11 studies with 949 total patients where persistent UI was found to be 12.1% in non-RT patients and 29.5% in post-RT patients, which yielded a statistically significant risk ratio of 2.08 [4]. However, it must be noted that there was an absence of standardised pad tests and patient-reported outcomes in various studies.
In such cases of persistent UI after AUS implantation, further investigations need to be performed to evaluate the cause of the incontinence. This involves a urethroscopic examination and a urodynamics study. If there is detrusor overactivity present, pharmacologic management, such as anticholinergics or beta-3 agonists should be started as first line therapy.
For patients with severe urethral atrophy or recurrent erosion, more advanced surgical options like urethral augmentation techniques may be considered [23]. These are discussed in the following sections.
Some authors have reported the use of lower pressures by decreasing fill amount in the pressure regulating balloon (PRB) for patients who are post-RT. It is hoped that such lower pressures may reduce the risks of urethral atrophy [4]. On the other hand, other authors have instead described using higher pressures PRB (e.g. using 71-80cmH2O instead of 61-70cmH2O) to assist in better urethral coaptation in cases of persistent UI due to urethral atrophy [24 & 25]. To our knowledge, there is no high-level evidence in modifying PRB pressures for patients who are post-RT. This, coupled with the difficulty in surgical access of the PRB and risk of infection [24], have limited its wide-spread adoption.
Management of Urethral AtrophyUrethral atrophy, characterized by the thinning of the urethral tissue surrounding the cuff, is another common complication for post-RT patients who have had AUS implanted. The options for managing urethral atrophy generally include downsizing the cuff, repositioning it proximally or distally to a healthier urethral segment, TC cuff placement, or using additional surgical techniques such as interposition of tissue grafts or the Gull-wing technique [26].
Cuff DownsizingIn 2010, the 3.5 cm AUS cuff was introduced to address the problem of incomplete coaptation of the urethra in patients with urethral atrophy. Although there were initial concerns that a downsized cuff could lead to a higher risk of erosion, it seems that the erosion rates observed to date are comparable to those of larger cuff sizes when studied in a general population [28].
A retrospective study by Simhan et al. reported that 52% of 176 patients treated with a 3.5 cm cuff had a history of RT, and among these patients, 21% experienced cuff erosion [23]. In contrast, only 4% of non-irradiated patients with the 3.5 cm cuff experienced erosion. The authors concluded that a history of RT was the only significant risk factor for 3.5 cm cuff erosion, with an odds ratio of 6.2.
It seems reasonable to conclude that the risk of AUS cuff erosion is significantly higher in patients with prior pelvic RT. While AUS erosion could happen regardless of cuff size, it would be prudent for urologists to note that about one-fifth of post-RT patients who had 3.5 cm cuffs could experience urethral erosion. Cuff size of > 3.5 cm on the other hand, was not seemingly associated with an increased risk of erosion or atrophy [29]. Precise spongiosal measurement and cuff selection are therefore crucial components of successful AUS placement, particularly among these high-risk patients.
Transcorporal ApproachThe transcorporal (TC) approach addresses the challenges associated with compromised urethral tissue, particularly in patients with urethral atrophy or previous eroded AUS implant. This technique involves placing the AUS cuff within the corpora cavernosa, providing additional support and reducing the risk of urethral erosion [15]. Bilateral incisions are made in the tunica albuginea of the corpora cavernosa to create a tunnel for the AUS cuff. These incisions are typically 2 cm long. The cuff is then placed within the corpora cavernosa, posterior to the urethra. This positioning provides additional support and reduces direct pressure on the urethral tissue.
The TC approach has been associated with lower rates of major complications such as cuff erosion and infection. Redmond et al. (2020) reported that TC cuff placement resulted in a revision rate of 15% compared to 32% for the standard approach. Additionally, the erosion rate was significantly lower in the TC group (5%) compared to the standard group (20%). There was however no significant difference in patient satisfaction, continence or improvement rates as well as 90-day complication rates [30].
The TC approach is technically more complex than the standard approach and requires a high level of surgical expertise. There is also a potential risk of erectile dysfunction due to the manipulation of the corpora cavernosa. However, many patients who have had RP and RT usually have poor erectile function to begin with. This procedure may also be complicated to hematoma formation posterior to the urethra due to difficulty in completely suturing the corporal defects behind the urethra [31], which may eventually lead to infection.
The Gull-Wing TC modification has been previously reported, and involves creating a flap of tunica albuginea from the corpora cavernosa [32]. These rectangular flaps are raised and flapped onto the urethral segment ventrally, as a means to buttress the urethra prior to inserting the AUS cuff (Fig. 2). A similar sized xenograft or allograft is then used to cover the tunical defect of the corpora cavernosa. It is suggested that this technique offers extra protection to the urethra on its lateral and ventral surface, maintains the size of the corpora, and also creates a protective barrier separating the AUS from a potential future penile implant [32].
The tunica flap (TF) modification has recently been described [31], and involves passing rectangular shaped tunica flaps posterior to the urethra after sharp dissection of the midline septum. This allows suture closure of the corpora and is thought to reduce the risk of hematoma formation [31].
A retrospective study by Davenport et al. investigated the outcomes of using TC cuffs compared to the use of a 3.5 cm AUS cuffs in high-risk patients (defined as those with a history of prior erosion or urethroplasty) [26]. The authors reported that of 625 AUS patients, 59 received TC cuffs and 168 receiving 3.5 cm cuffs. 47% of patients with TC cuffs experienced urethral erosion, as compared to 15% of patients who were given 3.5 cm cuffs. Multivariate analysis confirmed that TC cuffs were significantly associated with increased odds of erosion (OR 6.65). The authors concluded that while TC cuffs could be used in high-risk patients, they were associated with higher erosion rates compared to 3.5 cm cuffs.
Use of Tandem CuffsThe use of tandem cuffs was first described in 1993 [27] and involves the sequential installation of two cuffs along the urethra to distribute the effective pressure of the urethral cuff across a broader surface area in order to achieve urethral coaptation [33]. In earlier publications, the tandem cuff has showed success in improving UI and maintaining high patient satisfaction, despite being a salvage procedure [33,34,35].
Eswara et al. investigated the outcomes of different AUS revision techniques [36]. They found that tandem cuff placement had the lowest rate of incontinence failure compared to the other methods. However, only 14% of the study participants were post-RT patients, and within this cohort, ‘cuff downsizing’ patients fared the worst. The authors postulate that the addition of a second cuff enhanced urethral resistance better than a single cuff, thereby improving continence outcomes.
Linder et al. conducted a retrospective review of 69 cases of men who underwent AUS revision for urethral atrophy [37]. Of these, 56 involved tandem cuff placements, 12 involved single cuff downsizings, and 1 involved cuff relocation. Approximately one-third of the patients had a history of prior RT. There was no significant difference in the 3-year overall device survival rate or the incidence of further surgery, erosion, and infection between both groups. The authors have also recommended reserving tandem cuff as an option after failed cuff downsizing [37].
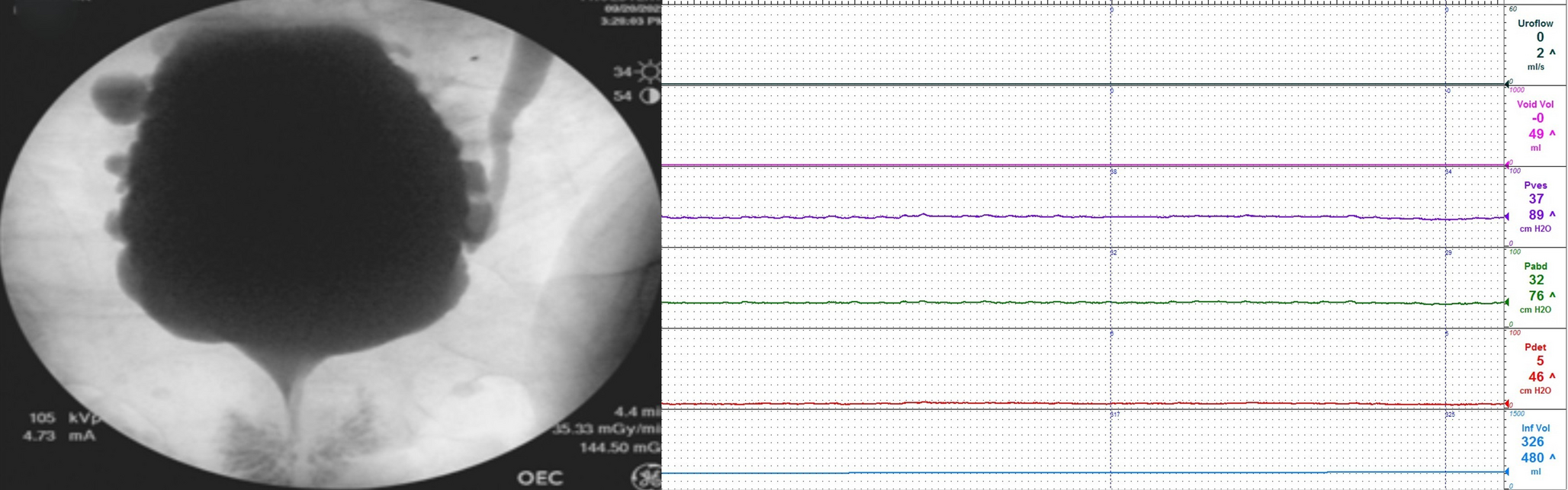
Mechanical Malfunction of AUS & Outcomes of Revision SurgeriesMechanical malfunction of the AUS device, including pump or cuff failure (Fig. 3), is an inevitable risk requiring device replacement or revision surgery. Common causes of mechanical malfunction include fluid loss from the system, pump failure, and cuff deflation. A recent study showed that the urethral cuff was the most common component to fail, followed by the PRB, tubing and lastly the control pump [38].
RT is thought to pose additional risks to the mechanical functioning of the AUS device due to fibrotic changes and reduced vascularity, which can lead to a more challenging surgical environment and higher rates of mechanical failure [14]. In addition, Loh-Doyle et al. reported that the 3.5 cm cuff, which is a common option for post-RT patients with urethral atrophy) had a statistically significant higher risk of failure (p < 0.01) compared to larger cuff sizes [38]. The site of the leakage was also commonly noted the site of a crease, which is a unique design feature of the 3.5 cm cuff [38].
A study by Rivera et al. examined the impact of prior RT on the survival and mechanical outcomes of AUS [29]. The research included 489 male patients with primary AUS implantations, of which 181 patients had received RT prior to AUS placement. The findings indicated that there was no significant difference in overall AUS device survival between patients with and without prior RT, with 1-year and 5-year survival rates of 92% vs. 90% and 77% vs. 74%, respectively. Despite the lack of a significant difference in device survival, the study highlighted that patients with prior RT were older, had higher BMI, and were more likely to have received androgen deprivation therapy [29].
Fig. 3
Comments (0)