Subjects and inclusion criteria
This study protocol was approved by the Human Research Ethics Committee of the Faculty of Dentistry, Chulalongkorn University (project code: HREC-DCU:2019-090; date of approval: 4/17/2020) and complied with the Declaration of Helsinki. All subjects provided informed consent permission prior to study participation. This trial was registered on the ClinicalTrials.gov (http://clinicaltrials.gov), the number is NCT06231212, date of registration: 30/01/2024.
Firstly, subjects with TMD were screened at the Occlusion and Orofacial Pain Clinic at Chulalongkorn University Dental Hospital, and then recruited for this double-blind, randomized, placebo- and active-controlled clinical study. Inclusion criteria include subjects between the ages of 18 and 50 years, reporting TMD pain lasting for 30 days or less (acute pain), with pain ratings between 5 and 8 on a 0–10 numeric rating scale. The pain scale used ranges from 0, representing no pain, to 10, representing severe pain, with 1–3 indicating mild pain, 4–6 moderate pain, and 7–10 severe pain.
Participants who self-reported sleep bruxism or had any underlying chronic disease or undergoing any sort of treatment that may influence pain perception and/or inflammation, including diabetes, psychological distress, systemic inflammatory disorders, oral appliances, and medications were excluded.
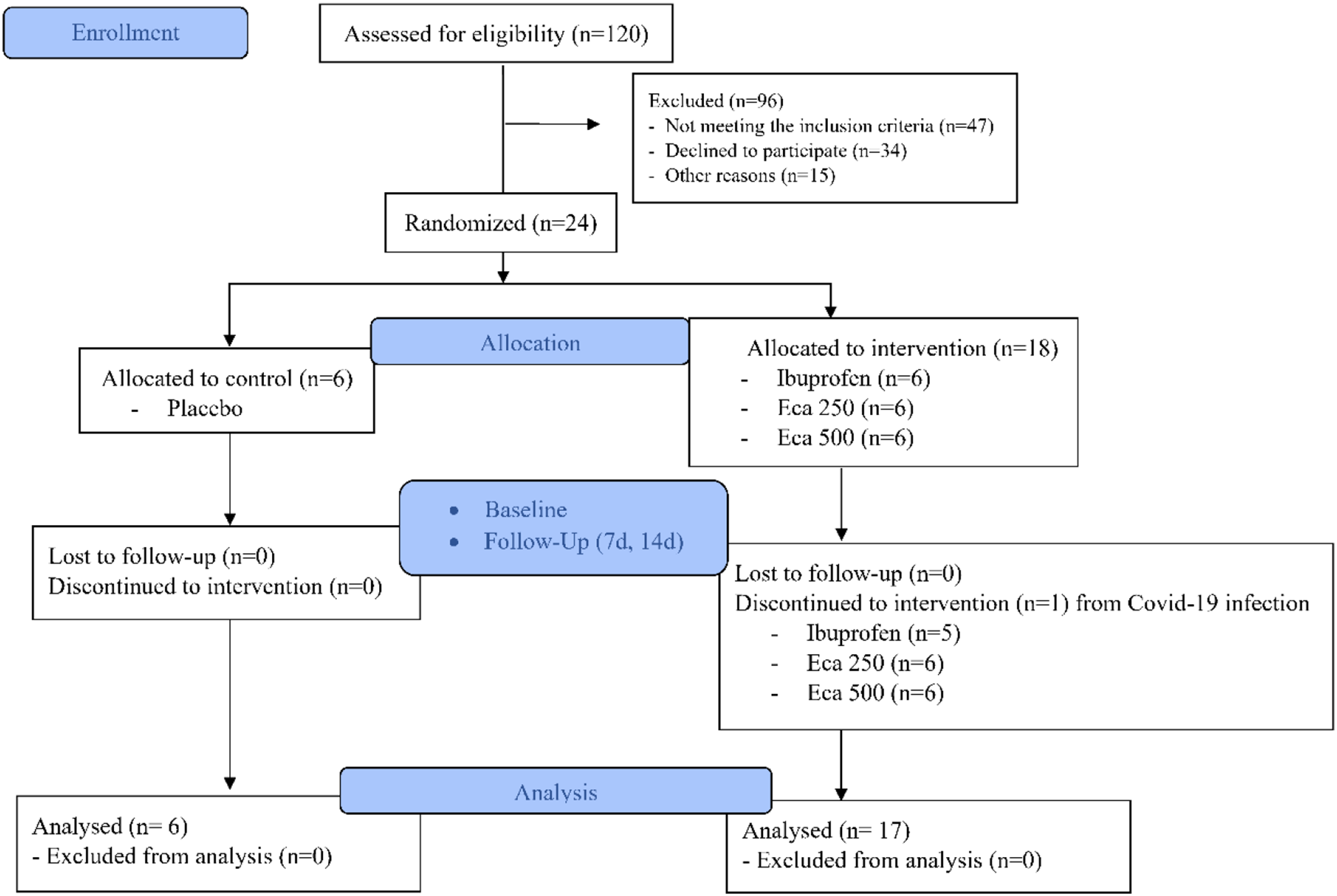
After enrollment, all subjects were diagnosed into two categories: the first group with muscle pain and the second with both muscle and TMJ pain according to DC/TMD axis I protocol [3, 12]. Then, the subjects received standard TMD self-care instructions [13] and received a pre-prepared, sealed, opaque packet containing the randomly allocated treatment groups. They were randomly allocated into four groups: (1) negative control group of 6 patients receiving a daily dose of 1,000 mg of lactose (placebo group); (2) positive control group of 5 patients taking a daily dose of 800 mg of ibuprofen (ibuprofen group); (3) the first ECa233 intervention group of 6 patients taking a daily dose of 250 mg of the active compound (ECa250 group) and (4) the second ECa233 intervention group of 6 patients taking a daily dose of 500 mg of ECa233 (ECa500 group). The active ingredients in the ECa capsules were pharmaceutical grade and sourced from Siam Herbal Innovation Ltd. (Lot No. MRA051401).
All subjects were requested to take the capsules of ECa233 twice a day in the morning and evening, after meals for 14 days. All capsules shared identical shape and color, manufactured in compliance with standard medical regulations and requirements, and successfully passed analytical tests conducted by Pharma Nueva Co., Ltd. They were stored at room temperature until prescribed. An identical lot of capsules were used throughout the experimental period.
The software G*Power 3.1.9.7 was used to analyze the sample size. An F-test (ANOVA, fixed effects, omnibus, one-way) was conducted, resulting in an effect size of 0.8. With an alpha error of 0.05, a power of 0.80, and four groups, the total sample size required was determined to be 24. As a result, six participants were established for each group.
Assessment of outcome variables via questionnaires and clinical examination
The self-reported pain intensity levels and other clinical parameters were collected at 3 time points: pre-intervention (baseline), 7- and 14-days post-intervention. The pain intensity score was determined by using a 10-point ordinal scale (0 representing no pain and 10 indicating severe pain). The clinical examination included the recording of the mandibular range of motion (ROM) in millimeters and the number of painful areas. These areas were evaluated upon palpation by a trained and calibrated senior clinician (P.P.) according to the DC/TMD criteria [3, 12].
A total of three mandibular ROM parameters were measured at pain-free, unassisted, and assisted mouth opening. Unassisted mouth opening was measured at the maximum distance regardless of pain or discomfort, whereas assisted mouth opening was performed with the assistance of the clinician. Afterwards, three further measurements were performed for each participant using a graduated metric ruler from the incisal edge of the right maxillary to mandibular central incisors.
Finally, the number of masticatory muscles and TMJs with pain upon palpation were quantified on both the left and the right side by the same calibrated examiner (initials). The total score of muscle pain was evaluated in the following locations using anatomical landmarks [3], temporalis muscles, masseter muscle, lateral pterygoid muscles, as well as the muscles around the posterior mandibular and submandibular region. Whereas the total score for TMJ pain was evaluated at the lateral pole of condyle.
Statistics
All data were tested for normality using the Shapiro-Wilk test. Data is presented as a mean ± standard deviation (SD), median and interquartile range (IQR) using the SPSS software (version 22, IBM, NY, USA). The Kruskal Wallis H test was used to analyze statistical significance between controls (placebo and active) and intervention groups. The Bonferroni correction was implemented. The Wilcoxon signed-rank test was used to evaluate the data within each group at 95% confident interval. The significance level was set at 5%.








Comments (0)