
Remember me
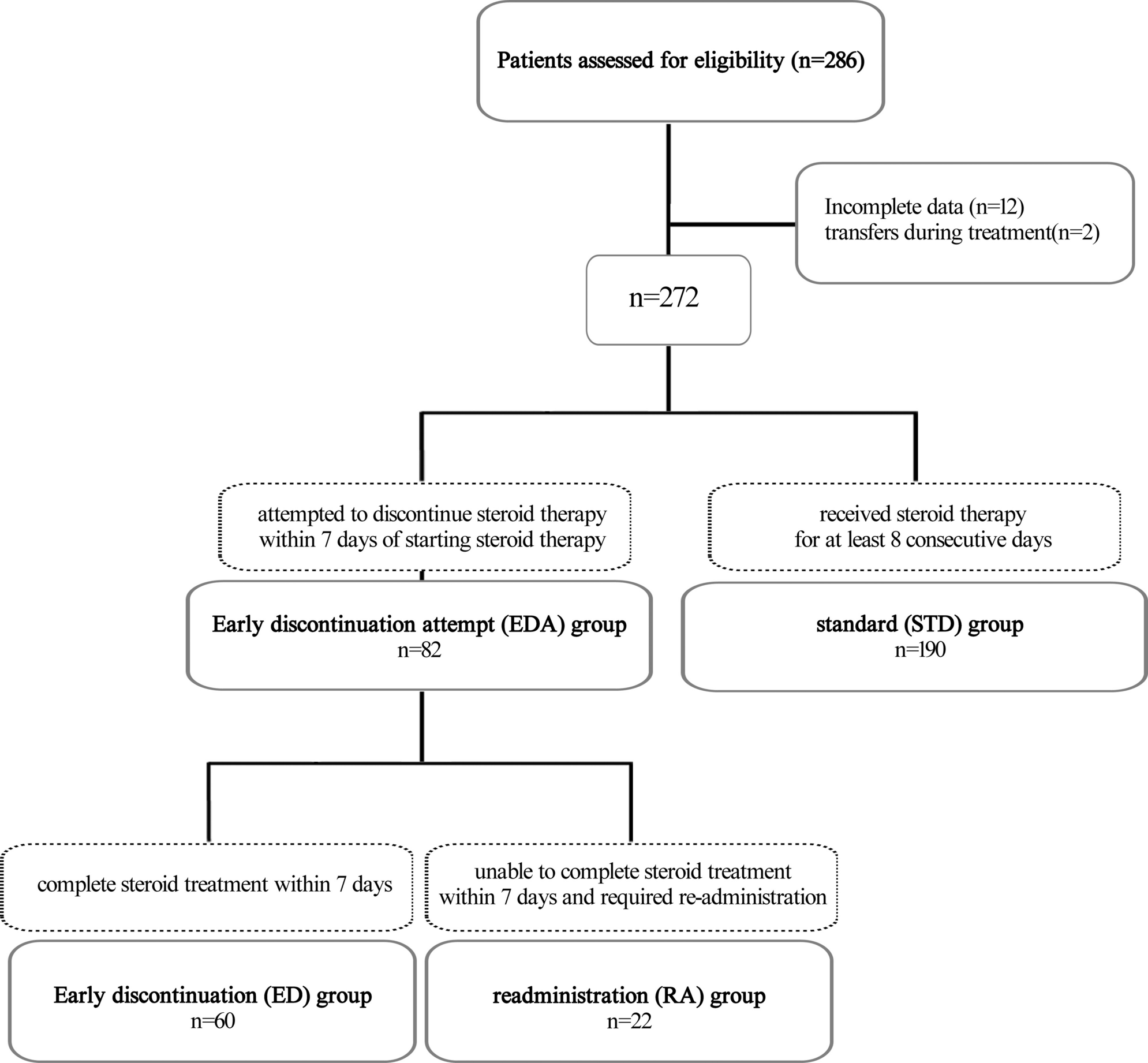

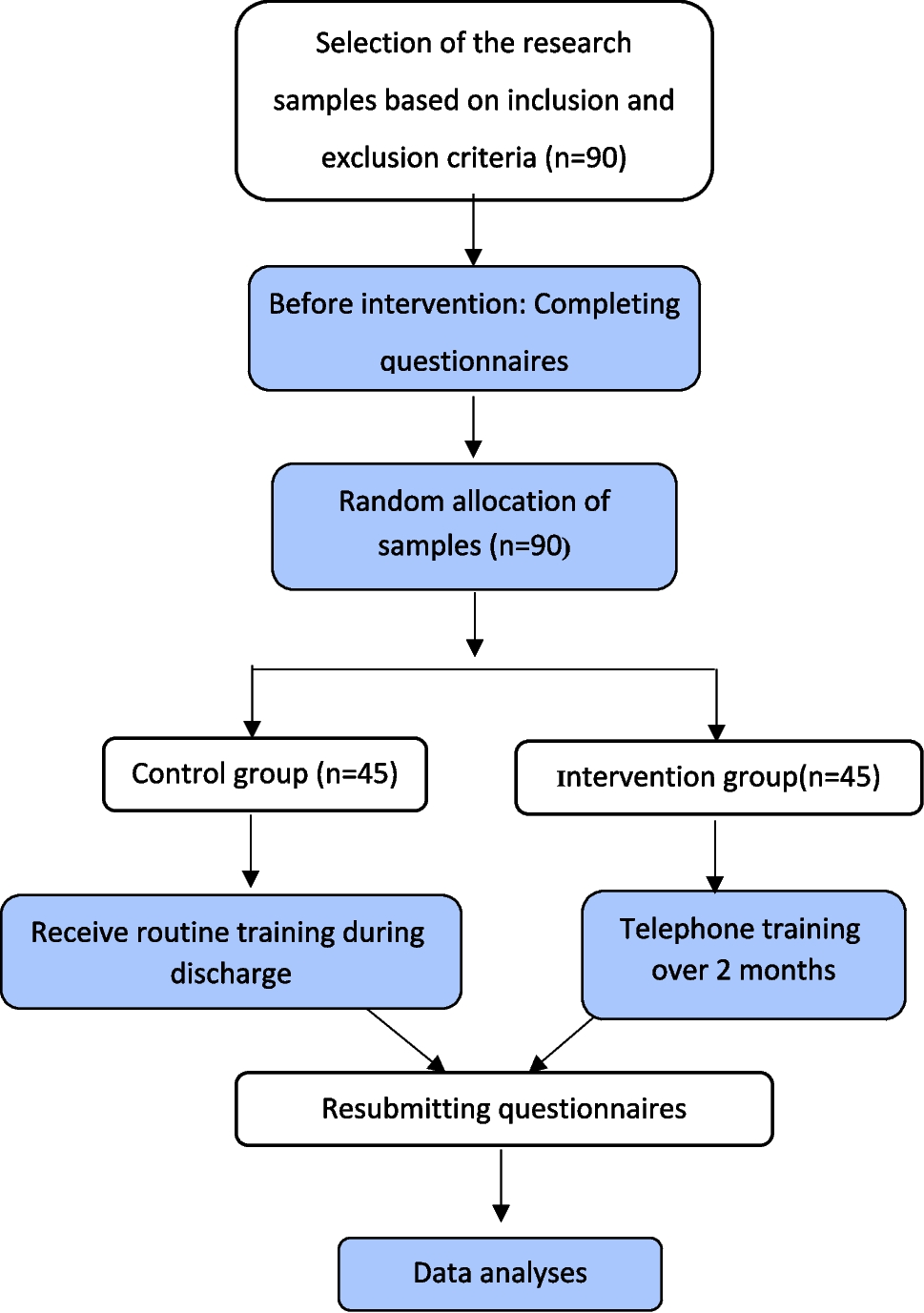

A total of 286 patients were initially included in the study, with 20 patients being excluded (12 with incomplete data; two transferred to other facilities during treatment). The remaining 272 patients were analyzed and divided into two groups: the EDA group (n = 82) and the STD group (n = 190) (Fig. 1).
Fig. 1
Flowchart of study patients
There were no significant differences in background characteristics, including age, gender, family history, medical history, or prior infection, between the EDA and STD groups (Table 1). In all patients, steroids were administered when abdominal pain was moderate to severe. The severity of abnormal pain and the presence of grossly bloody stools before steroid initiation did not differ between the two groups. Two patients in the STD group developed intestinal intussusception before steroid initiation, whereas none did in the EDA group. No patient in either group developed intestinal perforation. Blood and urine test results, including C-reactive protein and D-dimer levels, showed no significant differences between the two groups. Acetaminophen was used as a non-steroidal drug in 40 patients (48.8%) in the EDA group and 80 patients (42.1%) in the STD group. H2 blockers were used in 18 patients (22.0%) in the EDA group and 16 patients (8.4%) in the STD group. The median follow-up period was 175 days (range, 2–1857) in the EDA group and 215 days (range, 0–1873) in the STD group.
Table 1 Patient characteristicsTreatment outcomes in the EDA and STD groupsWe evaluated the impact of two steroid administration regimens on time to symptom resolution, length of hospital stay, steroid dosage, complications, and recurrence or relapse (Table 2). In the EDA group, the initial steroid dose ranged from 0.3 to 2.3 mg/kg/day (1–3 divided doses), with a median of 1.0 mg/kg/day. In the STD group, it ranged from 0.3 to 2.5 mg/kg/day (1–4 divided doses), with a median of 1.0 mg/kg/day. There was no significant difference in the number of days from steroid administration to the resolution of abdominal pain, grossly bloody stools, purpura, or arthritis or arthralgia between the two groups. However, the median length of hospital stay was significantly shorter in the EDA group (8.5 days vs. 15.0 days in the STD group, p < 0.01). Similarly, the total duration of steroid administration was significantly shorter in the EDA group (6 days vs. 17.5 days in the STD group, median, p < 0.01), and the total steroid dosage (PSL equivalent) was significantly lower in the EDA group (5.4 mg/kg vs. 15.4 mg/kg in the STD group, median, p < 0.01). Regarding severe clinical manifestations, there were two cases of intestinal intussusception in the STD group, but none in the EDA group. Both cases were successfully reduced using air or gastrografin enemas, and neither required surgery. There was no significant difference between the two groups in the incidence of intestinal perforation or severe renal involvement, recurrence, or relapse.
Table 2 Outcomes of the EDA and STD groupsSteroid-induced adverse events in the EDA and STD groupsWe examined whether different methods of steroid administration affected the incidence of steroid-induced adverse events. There was no significant difference between the EDA and STD groups in the occurrence of hypertension requiring treatment, ocular hypertension, hyperglycemia, or infections that may be associated with steroid use during treatment or within 4 weeks after discontinuation (Table 3).
Table 3 Steroid-induced adverse events in EDA and STD groupsSteroid readministration in the EDA and STD groupsTo determine whether an early attempt to discontinue steroids resulted in unfavorable outcomes, we subdivided the EDA group into two groups: the early discontinuation (ED) group and the readministration (RA) group, as defined in the “Methods” section. In the RA group, steroids were re-administered when abdominal pain worsened to a moderate or greater intensity after steroid discontinuation. Then, we compared outcomes such as total steroid dosage, duration of administration, length of hospital stay, rates of complications, and relapse/recurrence between the RA and STD groups.
Among the 82 patients in the EDA group, 22 patients (27%) required a second course of steroids due to the reappearance of abdominal symptoms shortly after the initial discontinuation (RA group), while the remaining 60 patients (73%) did not (ED group). Figure 2A shows the distribution of patients by total steroid dosage per body weight for the STD group, and Fig. 2B provides a similar analysis for the ED and RA groups. The total steroid dosage in the ED group was significantly lower than that in the STD group (4.7 mg/kg vs. 15.4 mg/kg, median, p < 0.01, Fig. 2C). Notably, the total steroid dosage in the RA group was also significantly lower than that in the STD group (8.6 mg/kg vs. 15.4 mg/kg, median, p = 0.02, Fig. 2C). The duration of steroid administration was also significantly shorter in both the ED and RA groups compared to the STD group (5 and 11.5 days vs. 17.5 days in the STD group, median, p < 0.01 and p = 0.01, respectively, Fig. 2D).
Fig. 2
Total steroid dosage and duration in the STD, ED, and RA groups. A Distribution of total dosage of steroids in STD group. B Distribution of total dosage of steroids in ED and RA groups. C Median total steroid dosage comparison. The RA and ED groups have lower median steroid dosage than the STD group. Data are presented as median (95% CI; confidence interval). D Median of total number of days on steroids. Both the RA and ED groups received steroids for fewer days than the STD group. Data are presented as median (95% CI; confidence interval). Patients in the ED and RA groups had lower total steroid dosage compared to the STD group. EDA, early discontinuation attempt; STD, standard; ED, early discontinuation; RA, readministration; *p < 0.05
There were no significant differences between the RA and STD groups in the length of hospital stay, incidence of severe clinical manifestations, recurrence, or relapse (Table 4). These findings indicate that even if early steroid discontinuation attempts are unsuccessful and readministration is required, patient outcomes are not adversely affected. Notably, early steroid discontinuation attempts led to reduced total steroid dosage and a shorter length of hospital stay compared to the STD group.
Table 4 Outcomes in the RA and STD groupsFactors that influence steroid dosageFinally, we analyzed factors influencing total steroid dosage. Patient background was not significantly associated with total steroid dosage (Table 5). Early discontinuation of steroids (EDA) was significantly associated with a lower total steroid dosage (5.4 mg/kg vs. 15.4 mg/kg in the STD group, median, p < 0.01). In contrast, the presence of grossly bloody stools and low Factor XIII were significantly associated with higher total steroid dosage. Specifically, patients with grossly bloody stools had a higher median total steroid dosage of 18.6 mg/kg (range 0.93–77.6) compared to 10.7 mg/kg (range 0.35–89.5) in patients without grossly bloody stools (p < 0.01). Factor XIII levels were inversely correlated with total steroid dosage, with a correlation coefficient of − 0.068 and a p-value of < 0.01, indicating that lower Factor XIII levels were associated with higher steroid doses.
Table 5 Effect of the factors associated with total steroid dosageMultivariate regression analysis confirmed that grossly bloody stools and low Factor XIII levels were significantly associated with an increasing total steroid dosage, while early steroid discontinuation was significantly associated with reduced total steroid dosage (Table 6). Specifically, a 10% decrease in Factor XIII increased total steroid dosage by 1.09 mg/kg, grossly bloody stools increased it by 5.34 mg/kg, and a short-term dosage EDA decreased it by 12.2 mg/kg.
Table 6 Multiple linear regression analysis
Comments (0)