
Remember me


The incidental finding of ectopic intrathyroidal thymic tissue in children is becoming increasingly common due to the widespread use of ultrasonography and this incidence is only expected to rise in the future. The clinical concern is that this finding is often misinterpreted as a thyroid tumour with a differential diagnosis of thyroid cancer and is communicated as such to the child and parents during the initial investigation which is usually performed by a non-specialist head and neck radiologist.
There is a huge disparity in management of this condition ranging from unindicated surgery resulting in medicolegal negligence claims to unnecessary long term follow up and/or FNA biopsies. There are no current guidelines or classification systems available to help manage this condition as most evidence is based on expert opinion. A better understanding of the natural course of both thymic gland development and involution in children and teenagers coupled with an equally good understanding of the risk of thyroid cancer in children is warranted. This knowledge would allow an age-dependent selective approach tailored to the individual patient avoiding unnecessary anxiety, overtreatment and/or intervention.
The UK National Clinical Consensus Guideline for paediatric differentiated thyroid carcinoma recommends “undertaking ultrasound-guided FNA on a thyroid nodule reported on ultrasound as U3 — indeterminate, U4 — suspicious or U5 — malignant” [6]. Although FNA is considered a safe and minimally invasive procedure, it carries a small risk of haematoma, and often requires a general anaesthetic to accurately target the lesion, and its associated risks, in the paediatric population.
We studied 21 children who were diagnosed with incidental ectopic intrathyroidal thymic tissue. The majority of patients were referred from other centres to our unit to perform an FNA biopsy to rule out a thyroid cancer. This has been the information communicated to the patient and the parents at the time due to lack of knowledge of a possible benign intrathyroidal thymic entity.
Accurate anatomical imaging by highly skilled head and neck radiologists is key in making a thorough assessment but other individual patient factors also need to be considered. Most important of these are patient’s age, personal and family history and access to previous ultrasound scans for comparison which is sometimes a logistical issue with distant referrals. The age of the child at presentation would be the most important determinant in our opinion. However, the upper age limit of children is often unclear but of significance in developmental endocrinology, as thymic gland development and involution are age-related. The UNISEF and the European union define children as persons under the age of 18 years while the American academy of paediatrics has gone a step further recommending an upper limit of 21 years for the paediatric population [7, 8]. Many clinicians would agree that the upper age limit should be at puberty. This would correspond well with endocrine pathophysiology and in particular, thymic involution. This inter-paediatric separation is not well-recognised by most hospital systems who would manage individuals under 18 years as one entity being admitted to the same wards, having access to same imaging services and treatment. It is our opinion and especially for thyroid cancer/thymus evaluation that pre-pubertal children should be separated from older teenagers and young adults.
Thyroid nodules in younger children are not common. The paediatric thyroid gland would not have gone through the chronic, low grade and intermittent TSH stimulation leading to hyperplasia and with time thyroid nodularity that is in part hormonally dependent, a feature lacking in pre-pubertal children. The medical concern here would be an underlying thyroid malignancy, most commonly PTC. It is also helpful to understand the difference in thyroid cancer incidence between younger children, especially the group where ectopic intrathyroidal thymic tissue is most common – in our series under 8 years with no one diagnosed over 10 years — and those who are older; teenagers and/or young adolescents who would still be classified as children by many societies. The UK cancer statistics for children, teenagers and young adults have reported that of 128 children diagnosed with thyroid cancer in 2021, only 13 (10%) were under the age of 14 years and only 3% were underage ten [9].
Most studies in the literature have not included details on children’s ages at the time of diagnosis but rather report on a mean age. None of the children > 10 years old or teenagers who were scanned at our unit had a diagnosis of intrathyroidal thymic tissue (420 ultrasound scans annually). Other studies have similarly shown that intrathyroidal thymic tissue is rare in older children; of the case series included [2, 5, 10,11,12,13,14,15,16,17,18,19,20,21] eight include children > 10 years old, and only one included children > 14 years old. The Fukushima Health Management Survey [3] found ectopic intrathyroidal thymus in 0.6% of participants aged 10–14 years and only 0.2% of participants aged 15–19 years, compared with 1.7% and 1.8% of those aged 0–4 years and 5–9 years respectively. Similar to our study, MH Bang et al. [10] reported on 16 children with intrathyroidal thymic tissue with none of the patients aged 10 or above.
The majority of reports of intrathyroidal thymic tissue in the literature are single case studies. Of the case series reported [2, 5, 10,11,12,13,14,15,16,17,18,19,20,21], the numbers of patients ranged from 2 to 42. These are low numbers and historically intrathyroidal thymic tissue has been considered rare. However, paediatric autopsy data [4] found thymic tissue in 9 (2.6%) of 350 thyroid glands, unrelated to cause of death of the child. Furthermore, the Fukushima Health Management Survey [3] found intrathyroidal thymic tissue in 375 patients with an incidence rate of 0.99%. This suggests that intrathyroidal thymic tissue is a common variant that will be increasingly incidentally picked up on ultrasound scan.
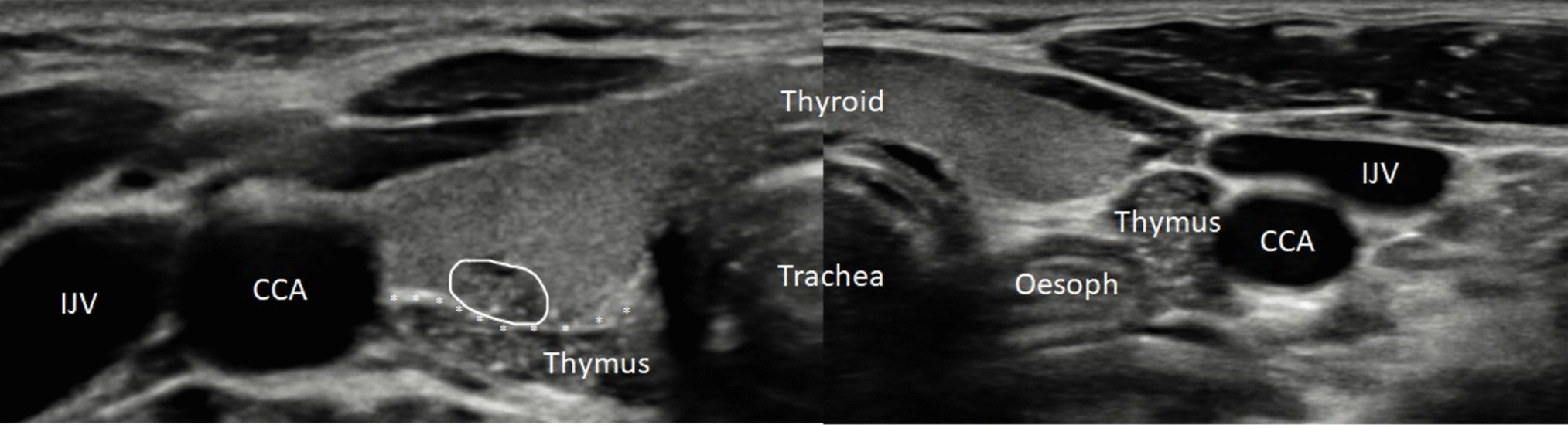
Alongside direct comparison with the thymus, there are sonographic features that may aid differentiation of ectopic thymus from PTC. Thymic tissue appears more hypoechoic than PTC; the echogenic foci in thymic tissue are brighter than those that represent microcalcifications in PTC; and intra-nodular blood flow on Doppler is less prominent in thymic tissue than in PTC [7]. This data suggests that the diagnosis can be reliably made in low-risk cases on the basis of sonographic features alone due to feasibility of comparison of the lesion to the patient’s own thymus which occurred in 90% of cases, with only three patients requiring an FNA.
Of the 12 patients who had follow up scans at our centre, all scans showed stable or improved appearances of the nodule: six were unchanged in size, three had slightly reduced in size, one was not mentioned in the report, and one demonstrated a slight increase in size. An eventual reduction in size is to be expected, in keeping with natural involution of the thymus. This is supported by Fukushima data [3] in which prevalence was inversely proportionate with age. Small increases in size are not necessarily cause for concern: the process of involution does not begin until puberty [22] so it would be logical to expect ectopic tissue to follow the same growth pattern.
There was one case of intrathyroidal thymic tissue which was detected on an ultrasound scan performed to assess presence of medullary thyroid cancer in a patient with MEN2 A prior to a prophylactic thyroidectomy. Evidence of intrathyroidal suspicious pathology in these patients would change the surgical strategy from a prophylactic to a therapeutic approach, unnecessarily escalating the extent of surgery to include a prophylactic level 6 lymph node dissection. Our group had previously shown that such an operation is correlated with a higher risk of postoperative hypocalcaemia [23]. The recognition of such an entity may avoid such complications in this group of patients, especially given that a prophylactic thyroidectomy would usually be recommended and performed in children under 5 years and occasionally under 10 years old.
There was significant variability in the time to the first follow up scan (1–22 months), duration of follow-up (1–39 months, median follow-up 6 months), and number of follow up scans (maximum 5). The first follow-up scan was generally recommended in either three- or six-months’ time. In three patients, no follow-up was recommended. This presumably reflects a confidence in benign appearances. There is no general consensus agreement on the frequency of the interval ultrasound scans required and/or for the duration these children would need to be monitored.
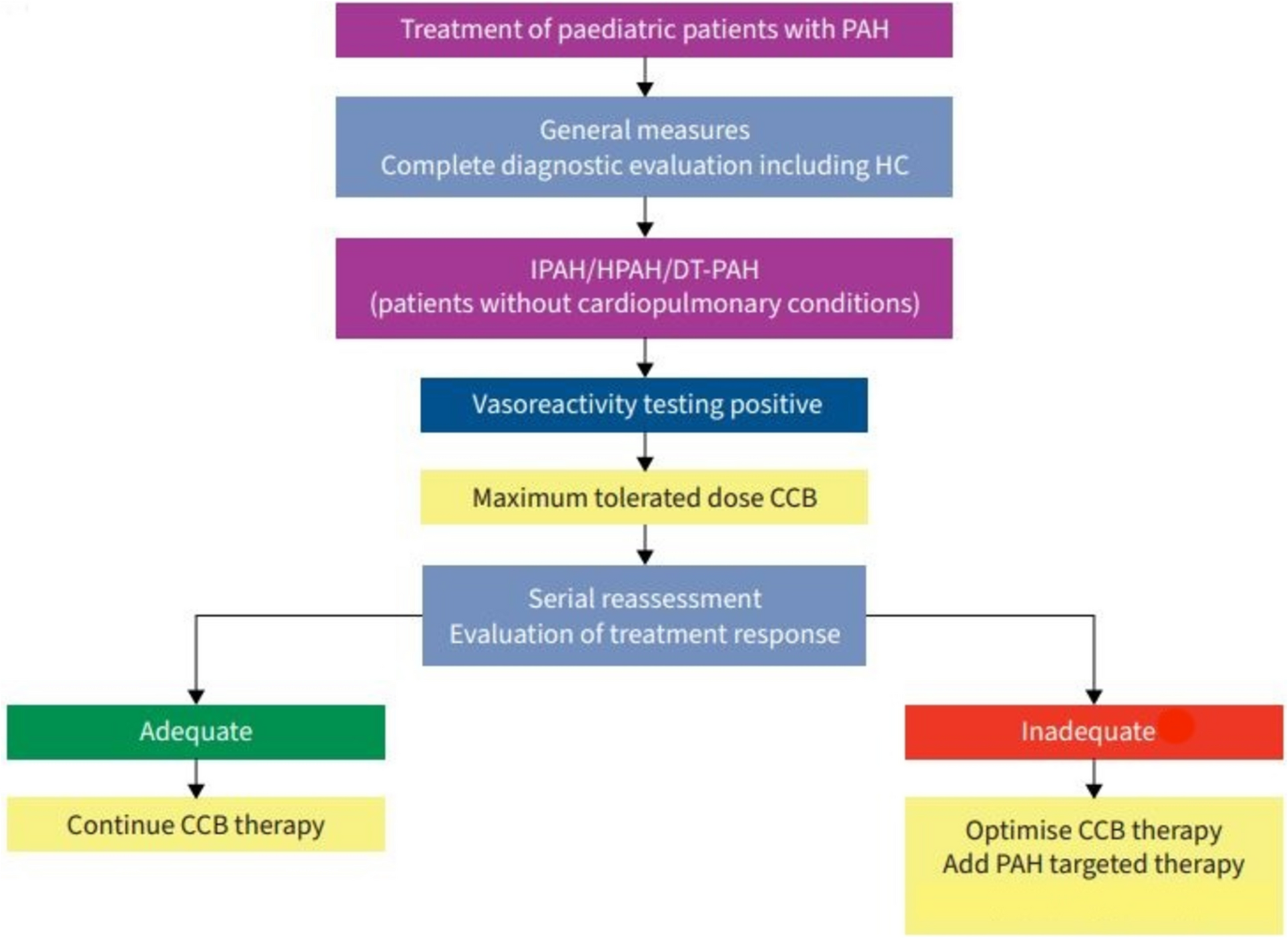
We would therefore recommend a separation of children with ectopic intrathyroidal thymic tissue into three groups based on age and the ability to compare directly with normal thymic tissue (Fig. 4). Children under 10 years old with availability of direct comparison to thymus and no relevant personal or family history and no concerning features in the history and clinical examination should not have an FNA biopsy and require no further ultrasound scans. Children between 10 and 14 years old would benefit from a repeat US scan in 1–2 years to assess and compare the stability or involution of the intrathyroidal nodule to the thymus. The third group > 14 years would require either regular interval scans or an FNA biopsy to exclude a thyroid cancer.
Fig. 4
Proposed management algorithm for paediatric patients with ectopic intrathyroidal thymic tissue
A limitation of this study is the low sample size, and a median follow up period of only six months, therefore this is a proposed stratification system which may be considered where there is no diagnostic uncertainty, and in patients without high-risk features. Further validation of this model in larger studies with longer follow-up duration is necessary to draw definitive conclusions regarding the safety of this approach.
In conclusion, this study highlights the need for increased awareness of intrathyroidal thymic tissue among clinicians and the need for a safe standardised diagnostic approach. It provides evidence for the safe use of surveillance scanning in low-risk paediatric patients with thyroid masses that resemble ectopic thymic tissue. Awareness among radiologists of this developmental variant and the value of comparison to normal thymic tissue to aid in its diagnosis has the potential to reduce parental anxiety and general anaesthetic required for FNA associated with tertiary referral for suspected thyroid malignancy. We propose a new classification based on age and visible thymic tissue to aid clinicians and radiologists make a decision on follow up and treatment.
Comments (0)